IBS diagnosis rests on symptom patterns, not a single lab result, scan, or stool test. For adults dealing with recurring abdominal pain, bloating, and bowel changes, that can be frustrating because the signs are real even when routine tests look normal.
IBS is a functional gut-brain interaction disorder, which means the bowel is working differently rather than showing one clear structural injury, and the goal is a clear path to diagnosis, red-flag review, and subtype sorting.
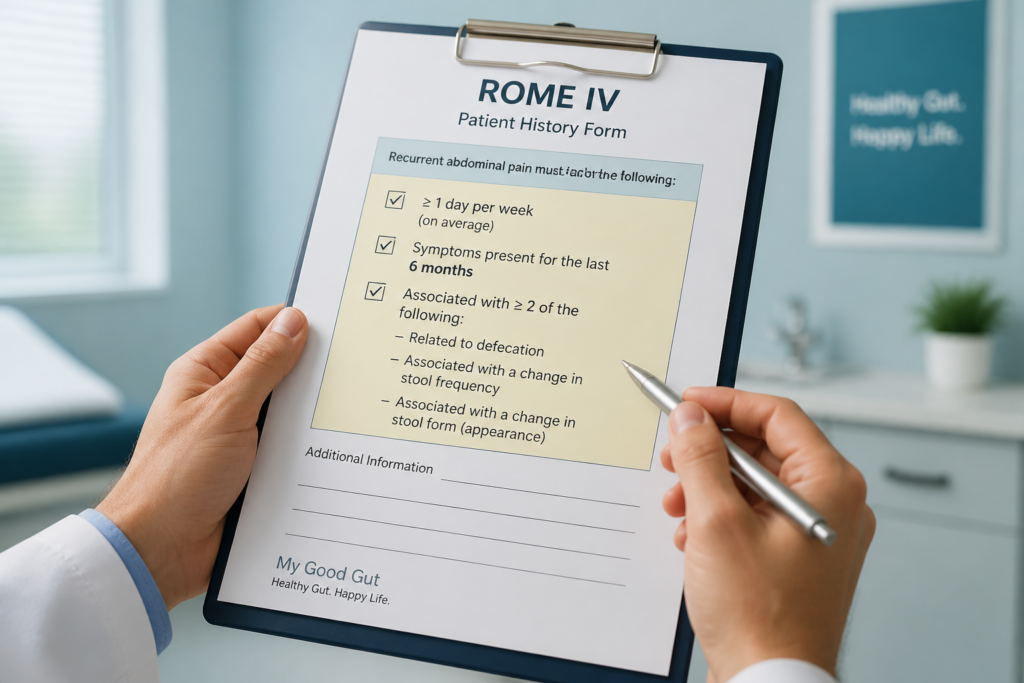
Rome IV is the main symptom standard clinicians use, and it looks for abdominal pain that happens at least 1 day a week on average, started 6 months ago, and links to changes in stool frequency or form, or pain related to bowel movements.
From there, the article covers which alarm signs shift the workup toward celiac disease, IBD, labs, stool markers, or colonoscopy, plus how the Bristol Stool Form Scale helps classify IBS-C, IBS-D, IBS-M, or IBS-U. It also gives a simple tracking method and a comparison with Manning and Rome III so the criteria feel usable in a real clinic visit.
For people living with ongoing digestive symptoms, and for caregivers trying to make sense of them, the most useful part is knowing when IBS fits and when it does not. A week of stool tracking can show a hard-lump pattern that points toward IBS-C, while bleeding, weight loss, fever, or nighttime diarrhea changes the plan fast.
My Good Gut keeps the focus on what matters in practice, so you can bring the right history to your clinician and move forward with more confidence.
IBS Diagnosis Key Takeaways
- IBS is usually diagnosed from symptoms and history, not one test.
- Rome IV requires recurrent pain, timing criteria, and bowel-related symptom links.
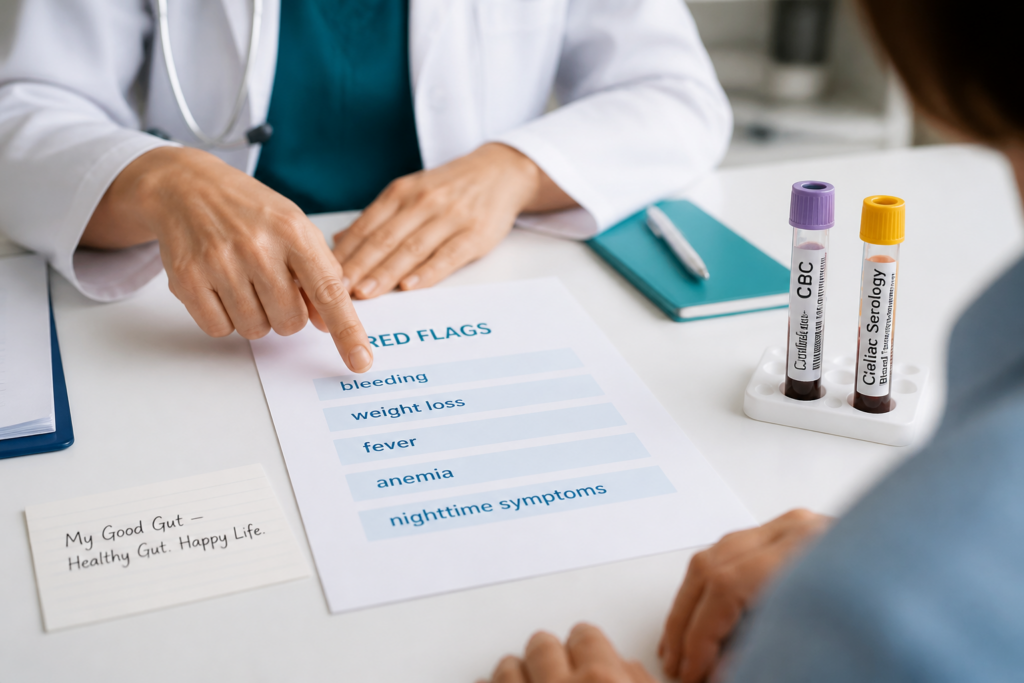
- Red flags include bleeding, weight loss, fever, anemia, and nighttime symptoms.
- Targeted testing can rule out celiac disease, IBD, or infection.
- Bristol Stool Form Scale helps classify IBS-C, IBS-D, IBS-M, and IBS-U.
- Track stool form on abnormal days to spot the dominant pattern.
- Manning and Rome III are older criteria, while Rome IV is current standard.
What Is IBS Diagnosis Based On?
IBS diagnosis results are usually based on your symptom pattern and medical history, not on one single blood test, scan, or stool result. Clinicians use the Rome IV criteria to recognize Irritable Bowel Syndrome, a functional gut-brain interaction disorder. In plain terms, the bowel can be more sensitive and work differently, but routine testing does not show one clear structural injury.
The usual pattern centers on recurrent abdominal pain. That pain is often linked to bowel movements and changes in stool frequency or form. Clinicians also look for defecation-related pain and ask whether the full symptom history fits IBS with enough confidence.
The clinical picture is often reviewed in a simple way:
| Clinical question | What it helps sort out |
|---|---|
| Is there recurrent abdominal pain? | Supports IBS when it follows a clear pattern |
| Do stools change in frequency or form? | Helps confirm a bowel pattern and subtype |
| Are there red flags or other clues? | Signals whether another condition needs closer review |
IBS is usually diagnosed from symptoms and history, but other likely causes should be ruled out when the pattern does not fit typical IBS (source). Celiac disease and inflammatory bowel disease are especially important. Targeted testing can be appropriate when symptoms or risk factors point elsewhere, but broad testing is often unnecessary. diagnosing IBS explains why that approach can save time and limit extra testing.
That matters because symptom-based diagnosis can reduce unnecessary tests, speed up the IBS diagnosis, and get you into symptom management sooner. It also helps you and your clinician focus on the right red flags, including unexplained weight loss, bleeding, fever, or a family history that changes the plan.
How Does Rome IV Diagnose IBS?
Rome IV criteria are the symptom-based standard clinicians use for an IBS diagnosis. They focus on recurrent abdominal pain, not on a single test result.
The timing has to fit a clear pattern. Rome IV defines IBS as recurrent abdominal pain on average at least 1 day per week in the last 3 months, with symptoms that began at least 6 months before diagnosis (source). That window helps separate IBS from short-lived stomach upset.
The pain also needs to connect with at least two of these three changes:
- Defecation-related pain: The pain comes with or after a bowel movement.
- Change in stool frequency: Bowel movements become more frequent or less frequent than usual.
- Change in stool form: Stools become harder, looser, or less predictable.
A quick way to apply the rule at the point of care is to match the history against all three parts at once. If the frequency, the duration, and at least two associated features line up, IBS becomes a stronger possibility.
| Rome IV piece | Plain-language meaning |
|---|---|
| Frequency | Pain happens about 1 day per week or more |
| Duration | Symptoms began at least 6 months ago |
| Associated features | Pain links to at least 2 of the 3 bowel changes |
Clinicians use Rome IV as the starting framework, then look for alarm symptoms and other causes that need more evaluation. Blood in the stool, weight loss, fever, anemia, or a sudden change in pattern can point away from IBS and toward another problem.
The Rome Foundation’s detailed guidance helps clinicians apply the Rome IV criteria in a consistent way. Even with that framework, persistent, severe, or changing symptoms still deserve personalized medical assessment. If your symptom pattern seems to fit, the next step is a careful review of the full history before the IBS diagnosis is confirmed.
Which Red Flags And Tests Matter Most?
Some symptoms need a closer look before you or your caregiver settles on IBS. If the pattern fits Rome IV and there are no alarm symptoms, a presumptive IBS workup is usually reasonable. Once common IBS red flags appear, the next step shifts from reassurance to targeted evaluation.
Common red flags include symptom onset after age 50, weight loss, rectal bleeding, fever, anemia, nighttime diarrhea or pain, and a family history of colorectal cancer or inflammatory bowel disease (source).
These alarm symptoms matter because IBS should not be the first explanation when the picture includes bleeding, anemia, or a later start in life.
When red flags or diagnostic uncertainty are present, clinicians often use limited testing such as a CBC, celiac serology, and inflammatory markers like fecal calprotectin or CRP to look for other causes (source).
Stool testing can help point toward inflammatory or infectious causes when the symptoms do not fit IBS. It cannot confirm IBS on its own, and it should not replace a broader evaluation when the story feels off.
Colonoscopy or another endoscopic exam becomes appropriate when red flags are present, when symptoms begin later in life without prior screening, or when bleeding, anemia, unexplained weight loss, fever, or ongoing nighttime symptoms raise concern for another diagnosis. Later-life onset without prior screening deserves special attention even if the pain and bowel changes seem familiar.
The simplest path is this: Rome IV symptoms plus no alarm symptoms usually support a presumptive IBS workup, while any red flag should move the plan toward labs, stool tests, and possible endoscopy. That approach helps you avoid missed diagnoses and unnecessary delay.
How Do Stool Patterns Classify IBS Subtypes?
The clearest way to sort IBS subtypes is to look at stool form on days when your bowel habits are abnormal, not on every bathroom trip. The Bristol Stool Form Scale scores stools from 1 to 7, and IBS subtypes are based on whether abnormal stools are hard or lumpy, loose or watery, or both on more than 25% of days (source). It often gives a clearer clinical picture than symptom labels alone.
The 25% rule is the key:
| Subtype | Stool pattern on abnormal days |
|---|---|
| IBS-C | More than 25% are hard or lumpy, and fewer than 25% are loose or watery |
| IBS-D | More than 25% are loose or watery, and fewer than 25% are hard or lumpy |
| IBS-M | More than 25% are hard or lumpy and more than 25% are loose or watery |
| IBS-U | IBS symptoms fit, but the stool pattern does not clearly match the other groups |
IBS-C means constipation is the main pattern. IBS-D means loose stools show up often, not just once in a while. IBS-M reflects an alternating pattern, with both constipation and diarrhea. IBS-U, or unclassified IBS, means your symptoms still matter even when the stool pattern is less distinct.
A simple tracking workflow can make the pattern easier to see:
- Track every bowel movement for at least 2 weeks.
- Score each stool with the Bristol Stool Form Scale.
- Count only abnormal stool days.
- Separate hard or lumpy stools from loose or watery stools.
- Use the 25% threshold to see which subtype fits best.
That kind of change in stool form over time is often what turns a vague symptom story into a useful IBS subtype.
How Do Manning, Rome III, And Rome IV Compare?
The Manning criteria were the first symptom screen. Rome III became the main symptom-based standard around 2006. Rome IV criteria are the version most clinicians use now when the symptom pattern fits IBS and alarm signs are absent.
| Criteria | Core idea | Practical effect |
|---|---|---|
| Manning criteria | A smaller set of symptom clues | More sensitive, but broader |
| Rome III | Recurrent abdominal pain or discomfort for at least 3 months, with symptoms starting at least 6 months earlier, plus 2 of 3 stool-related features | More structured and consistent |
| Rome IV | Tighter pain and timing rules | More specific and better at separating IBS from look-alike disorders |
That shift matters because each update narrowed the definition. Rome III was shaped by about 100 international experts and presented at Digestive Diseases Week under Dr. Douglas Drossman. Rome IV moved the field toward stronger clinical validation by reducing overlap with other functional digestive disorders and making symptom-based diagnosis more consistent in everyday practice.
The tradeoff is easy to remember:
- Manning criteria: catches more possible cases, but also more false alarms
- Rome III: balances breadth and structure
- Rome IV: sacrifices some sensitivity for better specificity
For frontline clinicians, Rome IV offers a practical framework after a careful history and red-flag review. If your symptoms meet Rome IV and there are no alarm features, that often supports an IBS diagnosis in routine care. Persistent, worsening, or unusual symptoms still need personalized medical evaluation.
IBS Diagnosis Criteria FAQs
These FAQs cover the basics of Irritable Bowel Syndrome, from stool form classification with the Bristol Stool Form Scale to how a bowel diary can help you spot patterns. They also address common questions about IBS-C, IBS-D, and where CBT may fit alongside a clinician’s evaluation.
1. Can doctors diagnose IBS from symptoms alone?
Yes, doctors can often diagnose IBS from your symptoms alone when you meet Rome IV criteria and do not have warning signs that suggest another condition, especially after a careful history review. IBS is not always a diagnosis of exclusion, so a positive, symptom-based diagnosis is often enough, though limited testing may still be used to rule out celiac disease or inflammatory bowel disease when symptoms are atypical. A meta-analysis of six studies found organic disease on imaging or endoscopy in about 1% of people who otherwise fit IBS criteria, which is why IBS colonoscopy is not always needed, and you should see a healthcare professional if symptoms are persistent, severe, or worsening.
2. How long must IBS symptoms last?
Rome IV says IBS symptoms should be present during the last 3 months, with symptom onset at least 6 months before diagnosis, and recurrent abdominal pain should occur on average at least 1 day per week during that 3-month window, which gives clinicians a timing benchmark. If your symptoms are newer or still changing, that doesn’t rule out IBS, but it usually means a clinician will keep watching the pattern and look more broadly for other causes first. The Rome Foundation’s Rome IV guidance is the standard reference for these timing rules and the related evaluation steps.
3. Is IBS diagnosed differently in children?
The core idea is the same in children, but pediatric clinicians usually rely on child-focused criteria and a careful history instead of adult-only rules, with extra attention to growth and daily function. IBS is still a diagnosis of exclusion, so they first look for other causes such as celiac disease or inflammatory bowel disease. Faster evaluation is important if there’s gastrointestinal bleeding, unexplained iron deficiency anemia, weight loss, or a sudden change in bowel habits, and you should see a pediatric clinician if symptoms persist or start affecting growth, school, or daily life.
4. Can stress or anxiety mimic IBS?
Stress and anxiety can trigger or worsen IBS-like symptoms through the gut-brain interaction, changing bowel speed, pain sensitivity, and urgency even when there’s no structural damage in the intestines, which can shape symptom flares. IBS is a functional gut-brain interaction disorder, so symptoms are diagnosed clinically, and stress may amplify them without meaning the cause is “just anxiety.” If you also have ongoing worry, poor sleep, panic, or avoidance around food or travel, both the emotional side and digestive symptoms may need care together. Persistent, severe, or worsening symptoms deserve medical evaluation so you can get the right diagnosis and a treatment plan that fits your bowel pattern.