IBS tests help rule out look-alike conditions, but they do not confirm IBS by themselves. For adults living with bloating, pain, diarrhea, or constipation, the hard part is often figuring out which tests matter and which ones only add cost and confusion.
IBS is usually diagnosed from symptoms, medical history, and a physical exam, and the right testing can point you toward safer next steps.
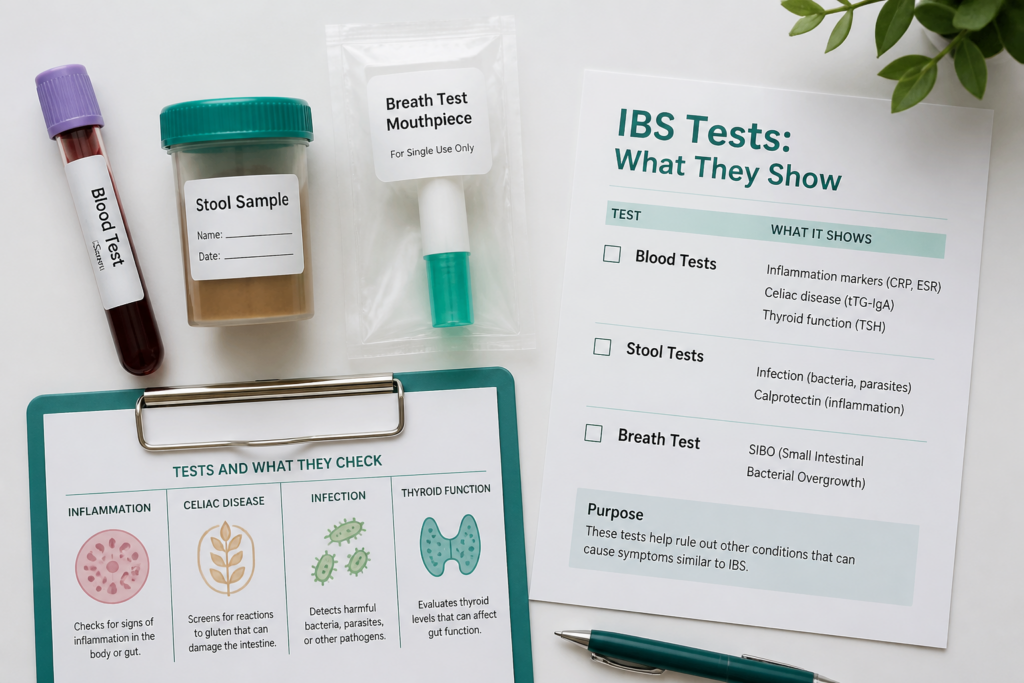
This article covers how blood tests like CBC, CRP, ESR, celiac serology, and TSH fit into the workup, along with stool tests such as fecal calprotectin and infection checks. It also explains when hydrogen breath tests can help, when colonoscopy is worth considering, and how red flag symptoms change the plan. Along the way, you’ll get a practical way to prepare for a GI visit, plus a simple checklist of what to track before testing.
For people with IBS, and for caregivers helping manage appointments, the main value is knowing how to ask better questions and avoid unnecessary testing. A patient with long-standing bloating and loose stools, for example, may need celiac blood work and fecal calprotectin before anything more invasive is considered. That kind of stepwise approach gives you a clearer path to answers and a calmer conversation with your clinician.
IBS Tests and Prep Key Takeaways
- IBS is usually diagnosed from symptoms, history, and exam, not one confirmatory test.
- Blood tests help rule out anemia, inflammation, celiac disease, and thyroid problems.
- Stool tests can detect infection or intestinal inflammation, especially fecal calprotectin.
- Hydrogen breath tests may help with SIBO or carbohydrate malabsorption.
- Colonoscopy is usually reserved for red flags or higher-risk situations.
- Red flags include bleeding, weight loss, anemia, fever, and nighttime symptoms.
- Good preparation includes symptom notes, trigger patterns, and test-specific instructions.
What Can IBS Tests Tell You?
IBS, or irritable bowel syndrome, is usually a clinical diagnosis. Your clinician starts with the symptom review for IBS, your medical history, and a physical exam. IBS tests can support that judgment, but they do not replace it. The IBS reference guide shows how that process fits together.
The main goal is to rule out other causes that can look like IBS, including inflammatory bowel disease (IBD), celiac disease, infection, thyroid disease, and, when age or risk factors make it relevant, colorectal cancer. These IBS tests help rule out IBD and other problems, but they do not confirm IBS on their own. Normal results make serious alternatives less likely. Abnormal results usually point toward a different explanation.
Common tests can still give useful clues:
| Test type | What it can suggest | What it cannot do |
|---|---|---|
| Blood tests | Inflammation, anemia, celiac disease clues, thyroid problems | Confirm IBS or an IBS subtype |
| Stool tests | Infection or intestinal inflammation | Diagnose IBS by itself |
| Hydrogen breath tests | Small intestinal bacterial overgrowth or carbohydrate malabsorption | Prove IBS is causing your symptoms |
That is why blood work, stool testing, and hydrogen breath testing are often used for bloating, diarrhea, constipation, and abdominal pain. A colonoscopy for IBS is not routine for everyone. It becomes more useful when red flags such as unexplained weight loss, rectal bleeding, or a family history of colon cancer are present. This stepwise path helps you avoid unnecessary procedures while still catching conditions that need treatment.
How Is IBS Diagnosed First?
IBS diagnosis usually starts with a symptom review for IBS, not a long test panel. Your clinician looks at bowel pattern, what happens after meals, diet, stress, and other health issues that could explain the symptoms. The IBS diagnosis criteria shape that first conversation, and they center on the Rome IV criteria.
In plain language, Rome IV defines IBS as recurrent abdominal pain at least one day a week in the last three months, with symptoms tied to bowel movements and changes in stool frequency or stool form (source). That pattern helps separate Irritable Bowel Syndrome from other digestive problems. It gives your clinician a clear starting point before testing gets broader.
Doctors will use the Rome IV Criteria’s Bristol Stool Scale to help determine the type of IBS that you have. There are 7 different types of stool on the Bristol Stool Scale:
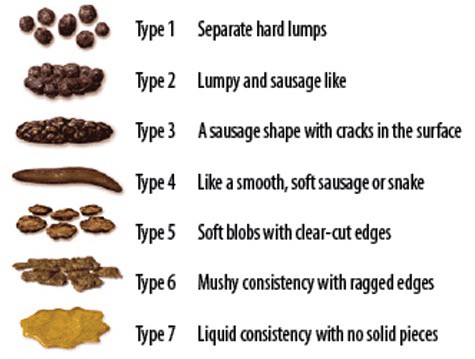
- If over 25% of bowel movements are type 1 or 2 and less than 25% are type 6 or 7, it’s IBS-C
- If over 25% of bowel movements are type 6 or 7 and less than 25% are type 1 or 2, it’s IBS-D
- If over 25% of bowel movements are type 1 or 2 AND over 25% are type 6 or 7, it’s IBS-M
- If none of the above, IBS-U (IBS Undetermined subtype)
A focused physical exam usually checks for:
- Tenderness: pain when the abdomen is pressed
- Bloating or swelling: a visibly distended belly
- Unusual lumps: anything that needs a closer look
Testing is individualized, too. Your age, IBS type you have, and whether your symptoms lean constipation-predominant, diarrhea-predominant, or mixed all shape the next step. Red flags push the workup further.
When symptoms do not fit the pattern, clinicians may order targeted tests. Clinicians may order a complete blood count, celiac serology, fecal calprotectin, hydrogen breath testing when small intestinal bacterial overgrowth is suspected, or colonoscopy when symptoms or alarm signs point to celiac disease, inflammatory bowel disease, or another cause (source, source).
The goal is to use your history and exam to avoid unnecessary testing while still finding the safest next step.
Which Tests Rule Out Other Conditions?
IBS tests are mostly about ruling out look-alike conditions. The aim is to rule out IBD, celiac disease, infection, and hormone problems with the fewest tests that fit your symptoms.
Common tests your clinician may order include:
- Complete Blood Count (CBC): This can show anemia or signs of infection.
- CRP or ESR: These inflammation checks can add support when inflammatory bowel disease is a concern.
- Celiac blood tests: Tissue transglutaminase antibody is a common first step, especially when bloating, diarrhea, weight loss, or an unusual symptom pattern makes celiac disease more likely.
- Thyroid-stimulating hormone (TSH): Thyroid testing can help when diarrhea points toward hyperthyroidism or constipation raises concern for hypothyroidism.
- Stool tests for infections: Stool cultures or parasite testing can find bacteria or parasites, while blood in the stool usually prompts a broader workup.
- Stool calprotectin and other fecal markers of inflammation: These help separate IBS from conditions like IBD.
Breath tests come in when bloating, gas, or diarrhea seem more intense than expected. Hydrogen or methane testing may point toward SIBO or carbohydrate malabsorption, and it helps to know whether it’s SIBO or IBS before settling on a plan.
Imaging or endoscopy is usually reserved for warning signs, not routine IBS care. Rectal bleeding, anemia, weight loss, older age at symptom start, or ongoing symptoms with no clear explanation can make a closer look necessary. A colonoscopy for IBS becomes appropriate when the picture is unclear or red flags are present.
How Do You Interpret Key Results?
Test results matter most when they fit the full picture. In IBS, clinicians look for patterns that point away from a simple functional gut problem and toward inflammation, celiac disease, infection, or another cause. Your stool frequency, stool appearance, symptoms, and alarm features all help make sense of the numbers.
| Result pattern | What it often suggests | Common next step |
|---|---|---|
| High stool calprotectin or other fecal markers of inflammation | Intestinal inflammation, not IBS alone | GI follow-up and more testing for IBD |
| Positive celiac serology, especially TTG-IGA | Celiac disease is more likely than IBS | Further celiac evaluation and diet guidance |
| Abnormal C-reactive protein (CRP) or ESR, anemia, or blood in stool | Inflammation, infection, or another organic cause | Broader workup, sometimes imaging or colonoscopy |
| Positive stool tests for parasites, harmful bacteria, blood, or inflammation | A specific infection or gut problem may be present | Treat or evaluate that cause instead of labeling it IBS |
| Positive IBS-Smart | Possible post-infectious IBS-D pattern | Interpret with symptoms and rule-out tests, not alone |
A high stool calprotectin result is an important clue. It usually means there is bowel inflammation, which makes inflammatory bowel disease more likely than IBS. Lactoferrin can point the same way. A positive celiac test works differently. It raises suspicion for celiac disease, while a negative result lowers the odds but does not explain every symptom by itself.
Blood work can also change the plan. Abnormal CRP, ESR, anemia, or stool blood usually push the workup toward something beyond IBS. Stool studies can also look for parasites, harmful bacteria, blood, and fecal markers of inflammation. If one of those is positive, the next step is usually to treat or investigate that specific finding.
Colonoscopy or extra testing becomes more likely if you have:
- Blood in the stool
- Unexplained weight loss
- Iron-deficiency anemia
- New symptoms after age 50
- A family history of colorectal cancer or IBD
When rule-out tests are normal, IBS becomes more likely. The full pattern still matters most, and your clinician uses the symptoms, alarm signs, and test results together to decide whether to reassure you, repeat testing, or keep looking.
How Do You Prepare for Common IBS Tests?
Good preparation makes IBS testing more useful and less stressful. A few notes from your own body help your clinician pick the right test and skip extra steps.
Before the visit, write down:
- Symptoms: what you feel, when it starts, how long it lasts, and whether bleeding, weight loss, fever, nighttime symptoms, or worsening pain show up.
- Patterns and triggers: diarrhea, constipation, urgency, or alternating stools, plus foods, stress, travel, illness, and medicines.
- Test prep: ask about eating rules for blood work, which medications or supplements should pause before breath testing, and how to handle stool or at-home kits.
For blood work, ask whether the panel includes CBC, CRP, ESR, celiac serology, or biomarker blood tests. Some clinicians also use IBS-Smart, which looks at anti-CdtB and anti-vinculin in certain people with IBS-D or post-infectious IBS. If you have an at-home blood kit, confirm the Tasso+ capillary blood device, prepaid return materials, and email results after the lab receives the sample.
For stool tests like fecal calprotectin, collect the sample exactly as directed, keep it sealed, and return it promptly. For hydrogen or methane breath tests, follow the fasting and diet plan closely because the results can help with lactose intolerance testing or SIBO-like symptoms. If you’re preparing for colonoscopy or upper endoscopy, follow bowel prep and fasting instructions exactly, since biopsy may help rule out celiac disease or other causes.
What Are Red Flags That Need Urgent Evaluation?

IBS red flags signal that your symptoms may not be IBS alone. Don’t wait for routine follow-up if you have unexplained weight loss, rectal bleeding, black or tarry stools, or iron-deficiency anemia. Those signs can point to bleeding or another problem that needs prompt testing.
A faster visit also makes sense when symptoms begin after age 50 or when a stable pattern changes. Fever, persistent nighttime diarrhea, or symptoms that wake you from sleep can point to infection or inflammation rather than IBS. A family history of colorectal cancer or IBD can move colonoscopy or flexible sigmoidoscopy higher on the list.
Common next steps include:
- Blood work: CBC, iron studies, CRP, or ESR
- Stool testing: fecal calprotectin or infection tests
- Endoscopy referral: colonoscopy or flexible sigmoidoscopy when bleeding risk or family history raises concern
If any of these warning signs appear, contact a healthcare professional quickly for urgent assessment and the right next test.
IBS Tests FAQs
These FAQs help you sort through how Irritable Bowel Syndrome is evaluated, what an IBS diagnosis usually means, and why Rome IV criteria matter. For related care options, our IBS treatment guide can help frame the next steps.
1. Can Any Test Confirm IBS?
No single test confirms IBS. Diagnosis usually comes from your symptom pattern, medical history, and criteria like Rome IV, while blood, stool, breath, and sometimes colonoscopy tests are used to rule out other causes such as celiac disease, IBD, infection, or inflammation. Normal results can still fit IBS, and they do not mean your symptoms are imaginary. Persistent, severe, or worsening symptoms should be checked by a qualified healthcare professional.
2. Which IBS Blood Tests Are Common?
Blood tests don’t confirm IBS, but they help rule out other causes such as infection, inflammation, anemia, celiac disease, or thyroid dysfunction. A CBC can show anemia or a high white blood cell count, which may point to bleeding, malabsorption, infection, or inflammation, while CRP and ESR can rise with inflammation, TTG-IGA can point to celiac disease, and TSH can suggest hyperthyroidism or hypothyroidism. Normal results support your IBS workup, and abnormal ones usually mean your clinician should look more closely for another explanation.
3. Do Stool Tests Check For IBS?
Stool tests do not diagnose IBS itself, but they’re often used to rule out other causes of diarrhea, pain, or bloating before IBS is confirmed. They can look for infection, parasites, harmful bacteria, blood, and inflammation, so stool tests for infections can point away from IBS and toward a different cause that may need treatment. Fecal calprotectin is especially helpful because higher levels suggest intestinal inflammation and make IBD more likely than IBS, while a normal result can support, but not prove, an IBS diagnosis when it matches your symptoms and other test results.
4. Are IBS Breath Tests Useful?
A hydrogen breath test can help with SIBO testing and lactose intolerance testing when your symptoms point to a clear trigger such as dairy or certain sugars. These hydrogen and methane breath tests are more useful as targeted tools than as a general IBS test, and the appointment can take up to 4 hours. Results may guide a diet change, but they do not confirm IBS, and false positives or mixed results can happen, so a short dietary trial may sometimes be the simpler first step if you and your clinician think it fits.
5. How Accurate Are IBS-Smart Tests?
IBS-Smart is a CLIA-certified, licensed, patented mail-in blood test that measures anti-CdtB and anti-vinculin antibodies, two biomarkers used in biomarker blood tests tied to IBS with a diarrheal pattern. It is designed for people with IBS-D and some cases of post-infectious IBS, so it is not a general test for every IBS type. The company claims “up to 100% positive predictive value” for its intended use, but it still supports evaluation rather than replacing a full medical assessment for ongoing digestive symptoms.

