SIBO and IBS are not the same condition, and the difference shapes testing, diet changes, and treatment choices. SIBO means too many bacteria are living in the small intestine, while IBS is a gut-brain disorder that changes how the bowel works. For adults, families, and caregivers dealing with bloating, gas, pain, diarrhea, or constipation, the goal is to sort out which pattern fits best.
This comparison covers symptom overlap, common causes, and the limits of testing such as breath tests and clinical criteria. It also shows when SIBO testing makes sense, when IBS can be diagnosed from symptoms, and which outputs help most, including red flag checklists, diet notes, and next-step questions for a clinician or dietitian. Clear guidance matters because the wrong assumption can lead to the wrong treatment plan.
That matters now because persistent digestive symptoms often sit at the center of daily decisions about food, work, and family routines. A person who gets rapid bloating after meals and low iron may need a different path than someone whose pain flares with stress and bowel changes, and one patient can have both patterns at once. Continue to the comparison so the next step is based on the symptom pattern, not guesswork.
SIBO vs IBS Key Takeaways
- SIBO is excess bacteria in the small intestine.
- IBS is a gut-brain interaction disorder.
- Both can cause bloating, gas, pain, and bowel changes.
- SIBO often causes fast post-meal distension.
- IBS diagnosis relies on symptoms and rule-out testing.
- Breath tests can help, but results have limits.
- Red flags like weight loss or deficiencies need medical review.
What Are SIBO And IBS?
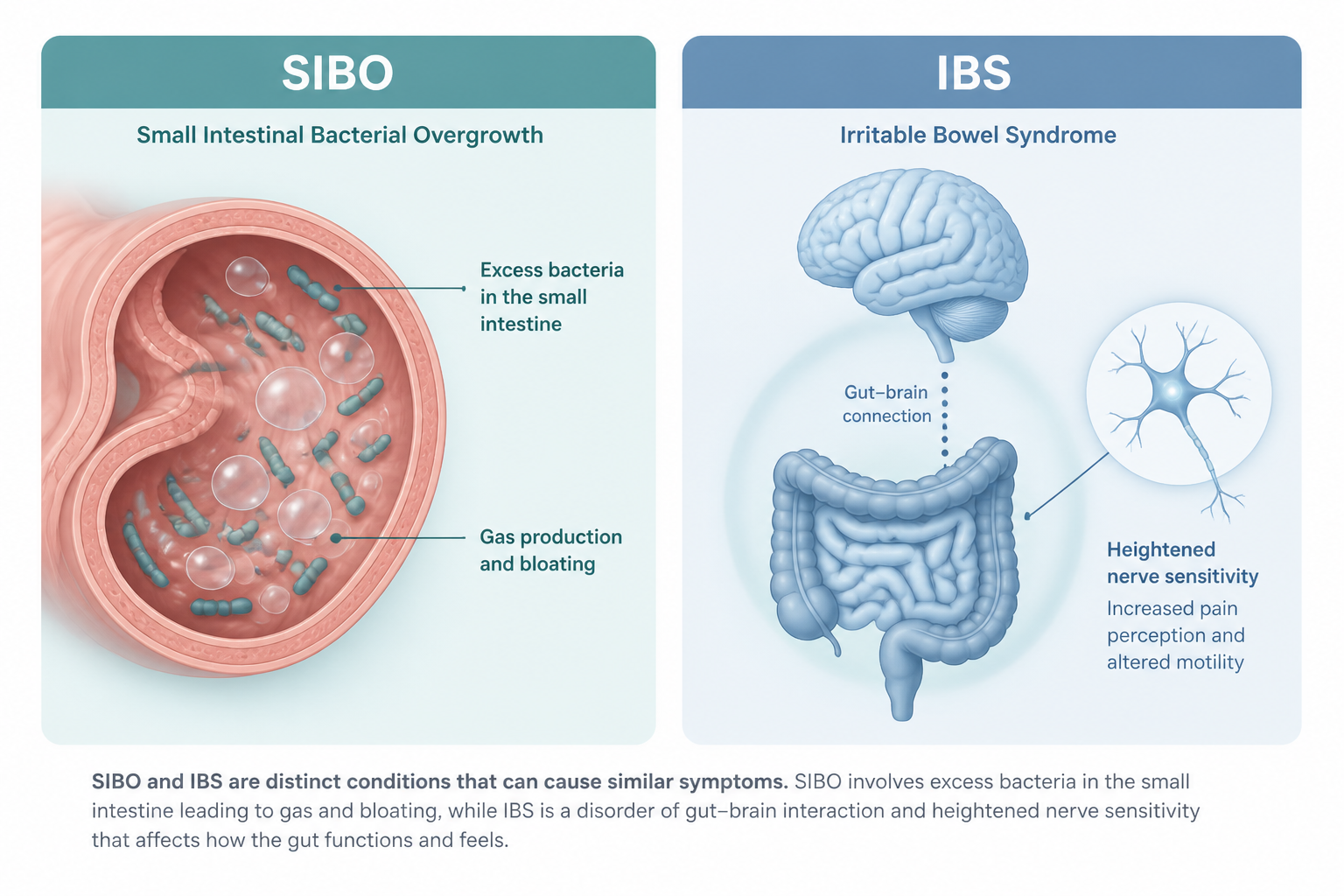
Small intestinal bacterial overgrowth (SIBO) means too many bacteria are living in the small intestine, where only a small amount should normally be present. That extra growth can cause gas, bloating, diarrhea, and constipation, and in some people it can also lead to malabsorption and nutrient deficiencies such as low vitamin B12 or iron (source). Irritable bowel syndrome (IBS) is different. It is a disorder of gut-brain interaction, so the digestive tract can look normal while still working in an abnormal way. That can lead to cramping, abdominal pain, bloating, gas, diarrhea, constipation, or a mix of these symptoms.
The core difference in SIBO vs IBS is the mechanism. SIBO is a physical and microbial problem. IBS is usually tied to altered motility, gut sensitivity, and changes in the gut-brain axis. That is why the two conditions are easy to confuse. Day-to-day symptoms overlap enough that symptoms alone cannot reliably separate one from the other.
This comparison matters because the next step depends on what is more likely driving your symptoms, or whether both are involved. Understanding how IBS is diagnosed is the starting point for ruling out other causes, but persistent or worsening digestive symptoms still deserve medical evaluation.
- SIBO: excess bacteria in the small intestine
- IBS: a functional gut-brain disorder
- Why it matters: testing and treatment are not the same
How Do Their Symptoms Compare?
SIBO and IBS can still differ in how those symptoms show up. Both can cause bloating, gas, abdominal pain, diarrhea, constipation, and mixed bowel habits. That overlap means SIBO symptoms and IBS symptoms are rarely enough to separate the two on their own.
The pattern gives you more useful clues. With SIBO, bloating after meals can feel tight or stretched, and abdominal distension may be more noticeable. IBS is often more pain-predominant (source).
Feature | SIBO | IBS |
|---|---|---|
Main pattern | More bloating and distension | More pain and cramping |
After meals | Fast swelling is common | Symptoms may flare, but less predictably |
Gas | Often heavier from early fermentation | Can happen, often with stronger pain sensitivity |
Common triggers | Food-related symptoms are common | Stress, anxiety, and certain foods often matter |
Bowel changes | Can include diarrhea and constipation | Can also include diarrhea and constipation |
The main difference is what drives the symptoms. In SIBO, bacteria ferment food in the small intestine and create gas in the wrong place. In IBS, a sensitive gut-brain system can turn normal stretching or gas into stronger pain, cramping, and urgency.
Stress-reactivity matters too. IBS often flares with stress or anxiety, while SIBO is more tied to fermentation and gas production. Some people have both conditions, which is why Irritable Bowel Syndrome and SIBO can be hard to sort out from symptoms alone.
If your abdominal pain, diarrhea and constipation, or rapid bloating after meals keeps coming back, a clinician or dietitian can help you look at red flags, testing limits, and your full history before you decide on next steps.
What Causes Each Condition?
The cause profile is straightforward. SIBO is a physical overgrowth problem in the small intestine. IBS is usually a functional condition shaped by gut-brain signaling, altered motility, and a more sensitive bowel.
Bacterial overgrowth in the small intestine develops when the bowel does not clear well or when the stomach barrier is weaker than expected. Slower gut motility, lower stomach acid, or easier bacterial migration can all play a part. Common drivers include:
- Medicines: long-term proton pump inhibitor or antacid use, recent antibiotics, and narcotic pain medicines
- Movement problems: gastroparesis and other forms of slow small-bowel clearance
- Structural issues: diverticulosis, adhesions, or prior surgery that creates a blind loop
- Other conditions: diabetes, scleroderma, and immunodeficiency
IBS usually has a broader and less visible cause pattern. The bowel may react too strongly because of visceral hypersensitivity, stress-related gut-brain disruption, mild inflammation, abnormal nerve signaling, and changes in how the intestines contract. The issue is often how the gut and brain communicate, not a fixed blockage or overgrowth.
A practical clue is that SIBO often points to a barrier or trigger problem, while IBS more often reflects gut-brain dysregulation. Both conditions can coexist, and that overlap can blur symptoms.
If you have ongoing bloating, gas, pain, diarrhea, or constipation, the pattern matters. Onset timing, medication history, prior surgery, and other health conditions can all help a clinician narrow the most likely cause.
How Do The Tests Differ?
SIBO is usually tested for, while IBS is usually diagnosed from symptoms plus tests like a colonoscopy to rule out other conditions. In IBS care, Rome IV criteria guide the diagnosis before more testing is ordered. A SIBO breath test looks for gases made when bacteria ferment sugar in the gut, usually hydrogen or methane.
Test or approach | What it measures | Main trade-off |
|---|---|---|
lactulose hydrogen breath test | Sugar that reaches farther into the small intestine | Can reflect rapid transit as well as overgrowth, which can raise false positives |
glucose hydrogen breath test | Sugar absorbed earlier in the small bowel | May miss more distal overgrowth |
jejunal aspirate culture | Direct small-intestine sampling | Invasive, costly, and still incomplete |
The main limit of breath testing is that it can measure orocecal transit time as well as bacterial overgrowth. That helps explain why different substrates, gas targets, cutoffs, and regional practices produce wide differences in reported SIBO rates in IBS studies. A positive result should be read with the full clinical picture.
The jejunal aspirate culture is more direct, but it is not a perfect gold standard. It samples only part of the small bowel, so a negative result does not fully rule out SIBO. A hydrogen sulfide breath biomarker may also appear in newer testing discussions, but access and interpretation are still evolving.
Testing should go beyond an IBS-style clinical diagnosis when you have severe early bloating after meals, unexpected nutrient deficiencies, unexplained weight loss, blood in the stool, worsening symptoms, or diagnostic uncertainty. Overlap is common, and SIBO shows up in a substantial share of people labeled with IBS. That overlap does not prove every IBS case is SIBO, so the right next step depends on your symptoms and exam, not symptoms alone.
How Do The Treatments Differ?
Treatment differs because the goal differs. With SIBO, care usually aims to reduce bacterial overgrowth directly. With IBS, care usually focuses on symptom relief, daily function, and fewer flares.
Area | SIBO | IBS |
|---|---|---|
Main first-line approach | Targeted antibiotics such as Rifaximin, often as a 14-day course | Symptom-based care with diet changes, stress support, and gut-directed therapies |
Evidence focus | Eradication and breath-test improvement | Symptom relief and quality of life |
Common add-ons | Combination regimens, other antimicrobials, or treatment of gut motility problems | Hypnotherapy, lifestyle changes, and medicines when needed |
Rifaximin is approved for IBS, but it is used off-label for SIBO. That difference matters because the treatment goals are not the same. In SIBO, meta-analyses report eradication rates of about 49.5 percent to 64.1 percent, and some reviews show antibiotics improve breath-test normalization versus placebo.
Some SIBO cases need a more layered plan. Clinicians may consider the elemental diet for SIBO, herbal antimicrobials for SIBO, or combination regimens when the case calls for it. Recurrent symptoms also raise the question of gut motility, and some people need prokinetics to prevent SIBO recurrence after treatment.
IBS care leans more heavily on the low-FODMAP diet, which means a low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols plan. The evidence is stronger for IBS than for SIBO, although it can still help recurrent bloating or pain under dietitian guidance. It does not replace treatment for true overgrowth or another root cause.
IBS also relies more on gut-brain therapies and day-to-day support:
- Hypnotherapy: may help lower gut sensitivity and stress-linked symptoms
- Stress management: can help you handle flares more steadily
- Lifestyle changes: can improve sleep, meals, movement, and routine
- Medications or neuromodulators: may help when pain or bowel changes need extra support
Probiotics and SIBO are a mixed area, so the best choice depends on your symptoms and diagnosis. Treating SIBO can improve IBS-like symptoms, but they often return if the original driver is still there. If your symptoms look like IBS but also point to SIBO, a careful evaluation can support a more durable plan.
How Can You Tell SIBO, IBS, Or Both?

SIBO and IBS can be hard to separate. Bloating, gas, abdominal pain, diarrhea, and constipation can show up in both, so symptoms alone usually cannot tell the difference. A symptom checklist is more useful than any single clue.
Clues that lean more toward SIBO include:
- Bloating after meals: swelling starts soon after eating.
- Heavy gas or visible distension: the abdomen looks noticeably larger.
- Malabsorption signs: unexplained weight loss or nutient deficiencies B12 and iron, plus low fat-soluble vitamins.
- Repeated lab changes: bloodwork suggests poor absorption rather than a short-term flare.
IBS tends to fit better when symptoms have lasted a long time without malabsorption. The Rome criteria for IBS focus on a pattern of recurring pain and bowel changes, not one test result. Pain that improves or worsens after a bowel movement, flares tied to stress or food changes, and otherwise normal testing all point more toward IBS symptoms.
Pattern matters more than one red flag. SIBO can cause abdominal pain from gas buildup in the small intestine. IBS can make normal stretching feel much more painful because the gut-brain system is extra sensitive. A 50-study systematic review found about 38% of people with IBS had evidence of bacterial overgrowth, so overlap is common.
A practical way to sort SIBO vs IBS is this:
- Ask about SIBO testing when bloating after meals comes with nutrient problems.
- Treat as IBS first when symptoms are chronic, stress-linked, and deficiency-free.
- Consider both when the picture is mixed, so malabsorption clues are not ignored and one bloating episode is not overread.
That balanced view can shape next steps like diet changes, antibiotics, gut-brain therapy, or an elemental diet for SIBO when a clinician thinks it fits.
Which Should You Suspect Next?
Your symptom pattern gives the first clue. Stress-linked flares, pain that comes and goes, and bowel changes that have been present for years fit IBS more closely. Severe bloating soon after meals, meal-triggered symptoms, or unexpected nutrient deficiencies make SIBO more suspicious, though overlap can happen.
If red flags are absent and the pattern stays steady, conservative IBS-first steps are a reasonable place to start. Track symptoms, keep meals regular, and make diet changes based on your own response instead of copying a one-size-fits-all plan. IBS red flag symptoms deserve a closer look if symptoms persist, worsen, or shift in a major way.
SIBO testing becomes more reasonable when bloating is pronounced, symptoms follow meals, or deficiencies appear. A hydrogen and methane SIBO breath test is the usual next step. The North American Consensus supports breath testing, and glucose versus lactulose testing can change what gets detected.
Specialist care makes more sense than more trial-and-error treatment when any of these show up:
- Unexplained weight loss
- Blood in stool
- Anemia or nutrient deficiencies
- Worsening or changing symptoms
- Diagnostic uncertainty
Antibiotics or antimicrobials may help when SIBO is present, but relief is not guaranteed. Symptoms can return if the underlying cause is still there.
Before your visit, use the My Good Gut checklist to note your main pattern, flag red symptoms, and write down questions about Rome IV criteria, SIBO breath testing, and next steps with a clinician or dietitian. This content is educational only and is not a substitute for personalized medical advice.
SIBO Vs IBS FAQs
These FAQs cover the most common SIBO vs IBS questions, including symptom overlap, testing limits, and what each diagnosis may mean for your next steps. They’re here to make the comparison clearer and feel a little less overwhelming.
1. What does a SIBO belly look like?
A SIBO belly is usually visibly swollen or distended, and the bloating often gets much worse after meals instead of staying mild or occasional. It can appear fast because bacteria in the small intestine ferment food early and create extra gas, which may leave you with pressure, tightness, or a noticeably larger abdomen. These SIBO symptoms are often more intense than ordinary fullness and may come with diarrhea, constipation, or both. With IBS, normal gas or stretching can feel much more painful, while SIBO tends to put gas in the wrong place.
2. Can you have SIBO without IBS?
Yes, you can have SIBO without IBS. The two can occur separately even though they often overlap. In a 50-study review, bacterial overgrowth appeared in about 38% of people with IBS, and broader estimates range from about 30% to 80% depending on the test and study group. SIBO is more likely to stand alone when symptoms begin after a clear trigger, such as a gut infection, surgery, slowed motility, or another condition that affects the small bowel.
3. Why is SIBO controversial?
SIBO stays controversial because the main tests are imperfect and do not always agree. The lactulose hydrogen breath test and glucose hydrogen breath test can miss cases or reflect transit time instead of true overgrowth, while jejunal aspirate culture is more direct but invasive and costly. Reported overlap with IBS ranges from about 30% to 80%, depending on the study. Rifaximin and herbal antimicrobials for SIBO may ease symptoms, but relapse is common if the cause remains. A hydrogen sulfide breath biomarker may help, yet no single standard approach exists.
4. Does SIBO ever fully go away?
SIBO can clear or improve after treatment, but it does not always stay away. Recurrence is more likely when the root driver is still present, such as slow gut motility, low stomach acid, or a structural issue that keeps the small intestine from clearing well. Antibiotics like rifaximin may ease IBS-like symptoms, but relief is not always a cure, and benefits can fade without follow-up monitoring. Durable management usually combines diet support with monitoring and, when appropriate, prokinetics to prevent SIBO recurrence, while the evidence for probiotics and SIBO remains mixed.
Sources
- Cleveland Clinic (source)
- Yale Medicine (source)
- PubMed Central (source)
- PubMed Central (source)
- NCBI Bookshelf (source)
- Gastroenterology & Endoscopy News (source)
- PubMed Central (source)
