IBS-M is the IBS subtype where bowel habits switch between constipation and diarrhea, and adults dealing with abdominal pain, bloating, and unpredictable stools need a clear next step. My Good Gut readers, especially busy working adults and families, can use a practical view of symptoms, triggers, diagnosis, and treatment to make sense of the pattern.
The sections below cover Rome IV symptom criteria, common triggers, red flags, and the tests that help rule out lookalike conditions. It also lays out low FODMAP food trials, soluble fiber, symptom tracking, and treatment choices that target the stronger side of the pattern without making the other side worse.
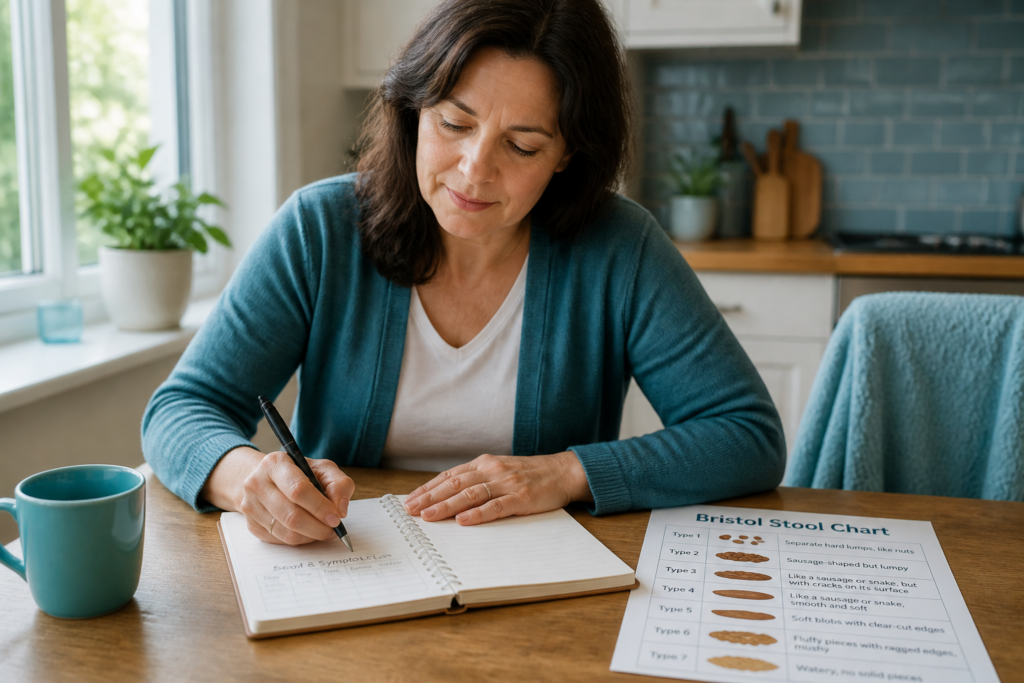
That matters now because mixed bowel habits can disrupt work, meals, travel, and sleep, and people often need plain guidance before they see a Gastroenterologist or Registered Dietitian Nutritionist. A simple stool log can show a pattern like hard stools for three days, then loose stools after one high FODMAP meal, which gives both patients and clinicians a starting point.
Keep going for a clear path from symptom recognition to more confident day to day management.
IBS-M Key Takeaways
- IBS-M alternates between constipation and diarrhea.
- Rome IV diagnosis depends on pain plus stool pattern changes.
- Red flags include bleeding, weight loss, fever, and nighttime diarrhea.
- Common triggers include high FODMAP foods, stress, alcohol, and caffeine.
- Low FODMAP trials and soluble fiber are common first steps.
- Treatment should target the stronger symptom without worsening the other.
- Symptom logs help guide clinician visits and personalized care.
What Is IBS-M And How Do You Recognize It?
Irritable bowel syndrome with mixed bowel habits, or IBS-M, is a type of irritable bowel syndrome (IBS) where your stool pattern shifts between constipation and diarrhea. It is often called IBS mixed because the bowel pattern changes over time, not just on a single bad day. The irritable bowel syndrome types page can help you place it in context.
Rome IV looks at stool form on abnormal-bowel-movement days, not just how often you go. More than 25% of bowel movements are hard or lumpy, which matches Bristol Stool Scale types 1 to 2, and more than 25% are loose or mushy, which matches types 6 to 7. Symptoms also need to fit IBS and not be better explained by medicine or another cause.
The pattern can feel inconsistent from week to week. Several days of constipation may give way to loose stools within the same week. That back-and-forth is what many people mean by alternating constipation and diarrhea and mixed bowel habits.
Common IBS symptoms often show up along with the stool changes:
- Abdominal pain
- Bloating
- Cramping
- A feeling of incomplete emptying
IBS-M differs from IBS-C and IBS-D because neither constipation nor diarrhea stays in control for long. A simple stool-and-symptom log can help you spot the pattern before a clinician visit, and an IBS subtype comparison can make the differences easier to see.
How Is IBS-M Diagnosed And What Must Be Ruled Out?
IBS-M is usually diagnosed from your symptoms and a careful check for other causes. There is no single blood test or scan that confirms an IBS diagnosis, so the goal is to match the pattern and rule out lookalike conditions efficiently.
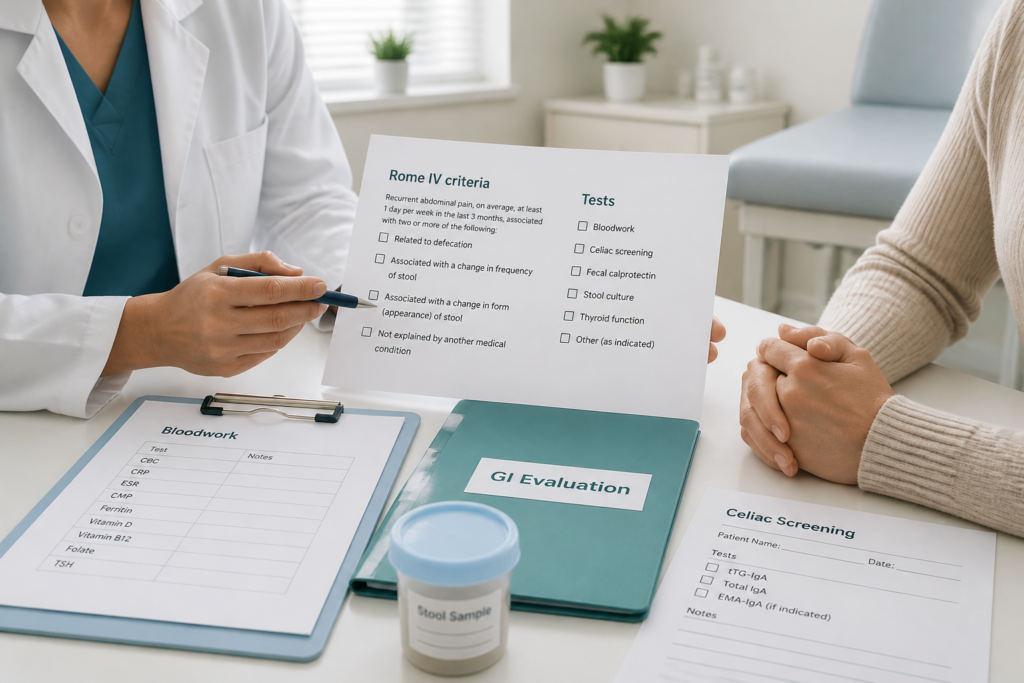
The Rome IV criteria guide that diagnosis. In plain terms, Rome IV diagnosis relies on recurrent abdominal pain that is linked to changes in stool frequency or stool form, with symptoms present at least 1 day per week in the last 3 months and beginning at least 6 months before diagnosis is considered (source). That pattern helps separate IBS mixed from short-term stomach bugs and other bowel disorders.
A clinician will also review the details that matter most:
- Pain history: when the pain began, how often it happens, and whether it changes after a bowel movement
- Bowel pattern: how constipation and diarrhea alternate, plus stool shape and urgency
- Triggers: foods, stress, travel, recent diet changes, and new medicines
- Medical clues: family history, personal history, weight loss, fever, bleeding, or anemia
A basic exam helps show whether IBS-M looks straightforward or needs more testing. Abdominal tenderness, dehydration, fever, pale skin, or unexplained weight loss can point to something other than IBS mixed.
Common first-line tests often include:
- Bloodwork: to check for anemia or signs of inflammation
- Celiac screening: to rule out gluten-related disease
- Stool tests: when infection, blood, or inflammatory bowel disease is a concern
- Fecal calprotectin: in some cases to look for intestinal inflammation
Colonoscopy, imaging, or endoscopy are not routine for every person. They are more likely if you are older, have red flags, or have abnormal test results.
Because there are no biological markers for IBS-M, the best approach is to confirm the symptom pattern and rule out mimics quickly. That helps you move sooner to safe first-step care and the right follow-up.
What Red Flags Need More Testing?
Symptoms that do not fit a typical IBS-M pattern need more testing, especially when they begin later in life or when warning signs such as bleeding, weight loss, anemia, fever, or nighttime diarrhea are present (source, source). A steady shift away from your usual ups and downs also deserves attention.
Urgent evaluation is more important when you notice these red flags:
- Visible blood in the stool
- Black, tarry stools
- Unintentional weight loss
- Fever
- Anemia
- Diarrhea that wakes you from sleep
- Symptoms that keep getting worse instead of fluctuating
These signs can justify blood work and sometimes a colonoscopy. The goal is to rule out serious causes before settling on an IBS diagnosis.
A practical differential usually starts with infection, especially when symptoms begin suddenly, after travel, or after antibiotic use. IBD and celiac disease matter when diarrhea, blood, weight loss, or family history are present. Watery diarrhea that keeps coming back also raises concern for microscopic colitis, medication-related diarrhea from NSAIDs, metformin, or some antidepressants, and bile-acid diarrhea. SIBO can overlap with bloating and bowel changes, but it should not distract from checking the more important causes first.
What Triggers IBS-M Flare-Ups?
IBS-M flare-ups usually come from a mix of things you can change and things you can’t. The goal is to spot patterns, not blame yourself. Genetics, inflammation, dysbiosis, and SIBO may all play a role, but those factors are not easy to control day to day.
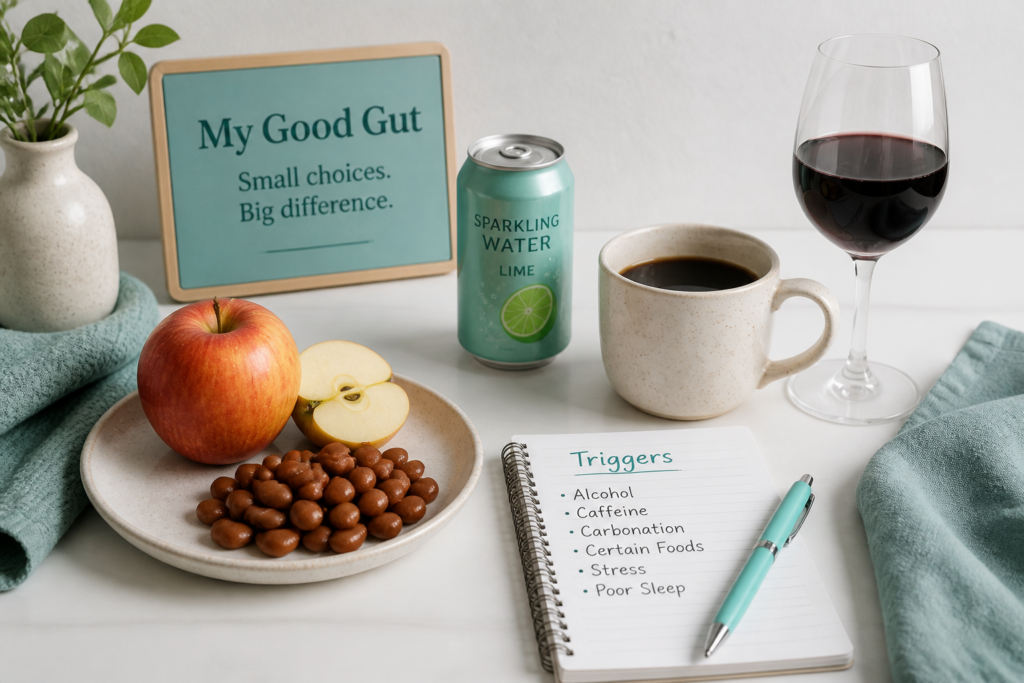
Common dietary triggers often show up first. High-FODMAP foods can pull extra water into the bowel and add gas, which may worsen pain, bloating, and stool changes. A low FODMAP approach can help you test these dietary triggers without cutting out everything at once. Many people also notice symptoms after dairy, fructose or sorbitol sweeteners, apples, cherries, watermelon, cabbage, beans, cauliflower, carbonated drinks, and raw fruits and vegetables.
Other flare-up triggers are worth watching too:
- Caffeine and alcohol: Coffee, energy drinks, wine, beer, or mixed drinks can increase urgency, cramping, and bathroom trips.
- Stress and IBS: Busy weeks, conflict, or emotional strain can amplify symptoms through the gut-brain axis.
- Infection or illness: A stomach bug can temporarily shift bowel habits.
- Medication changes: A new medicine can alter stool patterns or abdominal comfort.
Stress is not “all in your head.” The gut-brain axis links emotion, nerves, and digestion, so stressful periods can bring on constipation, diarrhea, bloating, or pain.
Tracking what happened before a flare helps you narrow the likely triggers and the timing. That pattern can guide first-step care and show when recent illness or medicine changes should be discussed with a clinician.
How Should You Treat IBS-M Without Worsening Either Side?
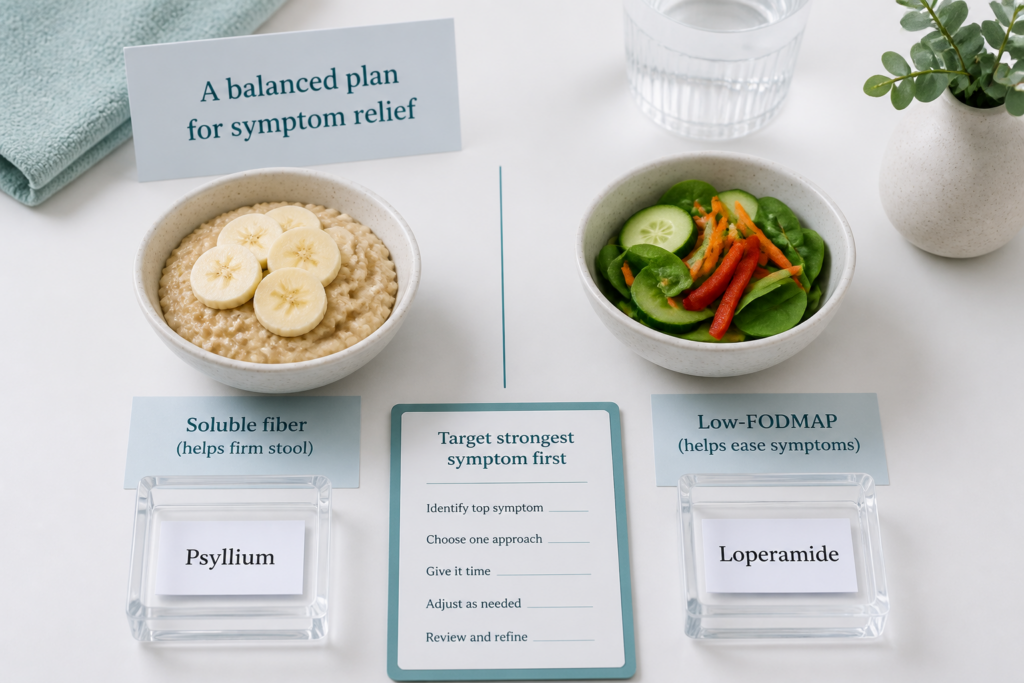
A good IBS-M plan starts by matching treatment to the symptom that feels strongest right now. When diarrhea is dominant, short-term control and cramp relief usually come first. When constipation is dominant, stool-softening support and fiber are the safer first moves.
| Current pattern | First moves | What to avoid if it makes the other side worse |
|---|---|---|
| Diarrhea-dominant flare | loperamide, fluids, antispasmodic medications for cramping | medicines that slow the bowel too much |
| Constipation-dominant flare | gentle laxatives, soluble fiber, hydration, movement | stronger anti-diarrheal use that can backfire |
Diet usually comes before medicine. A low FODMAP diet can help reduce pain, gas, and stool-related symptoms in some people with IBS, and peppermint oil may help abdominal pain and bloating (source, source). Food reintroduction matters too, because staying highly restricted for too long can make eating harder without adding more benefit.
Fiber works best as a balancing tool, not a one-size-fits-all fix. Soluble fiber is often the better starting point because it may help firm loose stools and soften harder stools at the same time. Insoluble fiber can be rougher for some people and may worsen bloating or urgency, so it often needs more caution.
Medication works best when it targets the active flare, not both problems at once. For diarrhea, diarrhea-predominant IBS can help frame when loperamide is the better fit. For constipation, IBS-C relief options can help you think through stool-softening choices before you add more medicine.
Clinicians may also consider rifaximin or low-dose neuromodulators for persistent symptoms, depending on the symptom pattern and the person’s medical history (source, source). The TARGET trials helped shape how clinicians think about these options.
The safest step-up rule is simple:
- If a treatment worsens the opposite symptom, switch strategies.
- If constipation gets worse, ease back on anti-diarrheal use.
- If diarrhea gets worse, scale down stool-softening tactics and ask about alternatives.
- If symptoms stay severe, change, or keep coming back, get individualized medical advice.
Digestive symptoms can have many causes, and responses vary a lot from person to person.
What Should You Try First?
Start with a steady baseline before you make bigger changes, then adjust one variable at a time. Regular meals, steady hydration, and a short list of likely triggers can help you avoid swings that push IBS-M toward diarrhea one week and constipation the next.
A simple first-line plan can look like this:
- Build routine: Eat at similar times each day and keep fluids steady.
- Try a brief low FODMAP diet trial: Work with a Registered Dietitian Nutritionist so the plan stays time-limited and includes reintroduction. Many people with IBS report symptom relief after finding the right mix of diet changes, fiber, stress care, and medication adjustments (source, source). The goal is to avoid staying overly restricted.
- Use soluble fiber carefully: Add it slowly, then watch for more bloating, looser stools, or harder stools.
- Track patterns: Write down stool form, pain, bloating, meals, stress, and flare timing in a food journal or symptom app.
- Add stress relief: Walking, yoga, meditation, or other relaxation habits can lower flare intensity.
- Consider OTC meds with care: Choose the symptom you want to calm first, and avoid overcorrecting one side of IBS-M.
This kind of self-management works best when you change one thing at a time and give your body a few days to show a pattern.
How Can You Manage IBS-M Day To Day?
A steady routine can make IBS-M easier to handle when constipation and diarrhea trade places. Start with a low FODMAP plan that uses guided elimination and reintroduction, then adjust portions and food choices based on the day’s symptoms. That helps you spot dietary triggers without cutting too much out for too long.
Simple self-management works best when it matches the pattern in front of you:
- During diarrhea flares: loperamide may help reduce stool frequency, but it should be used carefully so constipation does not swing back.
- During constipation flares: psyllium can support stool form and regularity, especially when you add it slowly with enough fluid.
- For cramping: antispasmodic medications such as dicyclomine or hyoscyamine may ease spasms. Persistent pain is a good reason to ask about peppermint oil or other options with your clinician (source, source).
Meals also matter. Smaller meals are often easier to tolerate than large ones, and steady fluid intake can help mixed bowel habits feel less unpredictable. Fiber sources that are easier to digest, such as oats, chia, kiwi, or cooked vegetables in modest amounts, may fit better than rougher or larger servings. If your symptoms stay hard to predict, a Registered Dietitian Nutritionist can tailor elimination and reintroduction so your plan stays flexible and realistic.
Non-food habits can calm the brain-gut cycle. Regular exercise, yoga, meditation, and a predictable daily rhythm may lower flare-ups during stressful weeks. Sleep hygiene matters too. Keep sleep and wake times consistent, and notice whether poor sleep lines up with more pain, bloating, or stool changes.
A simple symptom tracker or app can help you connect the dots. Record stool form, pain, meals, stress, and medication timing. If symptoms change, persist, or worsen, review the plan with a clinician. IBS-M self-management works best when it adjusts with your body over time.
How Do You Track Symptoms And Stool Patterns?
A simple record can make IBS-M patterns easier to spot. Track stool form with the Bristol Stool Chart in plain text. Record stool type, abdominal pain, bloating, meals, and stress so patterns are easier to review with a clinician. Use the Bristol Stool Scale as plain text if you prefer that wording.
Need one list. Let’s draft with no links. Must include all keywords plain text once.
No markdown link. Need no section heading. Let’s produce around 160 words. Ensure no prohibited sentence starts? You can/your allowed. Okay.
What Should You Expect Over Time?
IBS-M usually moves in waves. Your constipation and diarrhea can switch from week to week, and sometimes even within the same day or bowel movement. That makes early progress feel uneven.
The goal is symptom control, not a permanent cure. Some people notice improvement within weeks after a diet or medication change, while others need a longer period of trial and adjustment before they find what helps most (source, source).
IBS-M can also feel more painful or disruptive than a single-pattern IBS subtype. Even with a better baseline, flare-ups can still break through. Response is highly individual, so a food plan, fiber change, or medicine may help one person and worsen alternating constipation and diarrhea in another. Symptom tracking often makes your personal pattern clearer over time.
Follow-up is usually gradual:
- Diet changes: meals or fiber may be adjusted based on which bowel pattern is stronger
- Medicines: antidiarrheal or laxative use may shift with your symptoms
- Review visits: treatment plans are often refined step by step
If your symptoms keep changing, become more severe, or stop responding, seek reassessment. Persistent or worsening digestive symptoms need personalized medical review.
IBS-M FAQs
These FAQs cover the questions people most often ask about IBS-M, including how it fits under Irritable Bowel Syndrome and why IBS symptoms can change from day to day. The answers below help make mixed bowel patterns easier to recognize and discuss with confidence.
1. What Causes IBS-M?
IBS-M usually does not have one clear cause or a single biological marker, so diagnosis depends on symptoms and ruling out other conditions. The gut-brain axis can affect stress, pain sensitivity, and bowel nerve signaling, which may lead to alternating constipation and diarrhea. Dysbiosis, or an imbalance in gut bacteria, may also play a role, and some people notice symptoms after a stomach bug or infection, while genetics and low-grade inflammation may add to the mix.
2. What Is The Best Diet For IBS-M?
There isn’t one best diet for IBS-M, because your triggers can change from week to week. A supervised low FODMAP elimination and reintroduction plan is often the most useful first step, since it helps you find what you tolerate instead of staying restricted long term. Research has linked low FODMAP eating with symptom improvement in about 50% to 80% of people with IBS, but results vary, so it works best as a structured trial with a registered dietitian nutritionist. Track meals, symptoms, and stool pattern, then adjust fluids, soluble fiber, or easier-to-digest foods based on whether constipation or diarrhea is stronger.
3. Do Probiotics Help IBS-M?
Probiotics for IBS may help some people with IBS-M, especially bloating and abdominal pain, but the benefits are usually modest and not the same for everyone. Strains such as Bifidobacterium infantis and Lactobacillus plantarum have some supportive data, yet results depend on the exact strain, dose, and product, and evidence for IBS-M is still limited even in TARGET trials. A short trial can be reasonable, and products like IBgard may help some symptoms too, but they work best as one part of your plan, with diet and clinician guidance if symptoms persist or worsen.
4. Is IBS-M A Lifelong Condition?
IBS-M is often a long-term condition, but it does not stay the same for everyone. Your symptoms may settle for weeks or months, then flare again or even shift within the same day. There’s no permanent cure to promise, but steady attention to meals, stress, and bowel habits can improve control over time. If symptoms persist, worsen, or change in a concerning way, a qualified healthcare professional should check for other causes and help tailor your care.
5. How Long Do IBS-M Symptoms Last?
IBS-M flares often last a few days to a few weeks, but symptoms can shift from one day or week to the next, with constipation, diarrhea, or both returning after calmer periods. Some people improve in a few weeks, while others need months to find a routine that helps manage symptoms, and the long-term course can change with stress, diet, and other gut triggers. Seek re-evaluation if your pattern changes suddenly, symptoms get worse or more frequent, or you notice bleeding, weight loss, fever, or waking at night with symptoms, because persistent digestive symptoms can have many causes and this content is for educational purposes only and is not a substitute for personalized medical advice.
