An IBS subtype comparison helps people with IBS sort symptoms into IBS-C, IBS-D, IBS-M, or IBS-U so care matches the bowel pattern, not just the diagnosis. For adults and families who need clear next steps, that makes it easier to compare stool form, pain timing, and bowel movement frequency without guesswork. IBS is a digestive disorder with recurrent abdominal pain linked to bowel changes.
The rest of the piece covers Rome IV criteria, stool tracking with the Bristol Stool Scale, and how the 25% rule is used in subtype classification. It also reviews symptom logs, subtype-specific management, and when a clinician should reassess the pattern.
Readers get practical outputs like a simple stool diary framework, clearer subtype labels, and first-step treatment ideas for constipation, diarrhea, or mixed symptoms.
That matters now because busy people with IBS need plain language that turns symptoms into action instead of more confusion. A stool log can show whether hard stools, loose stools, or alternating patterns are driving the problem, and one week of tracking may reveal that a person who thought they had IBS-D actually fits IBS-M.
Read on to compare the subtypes and use the right next step for the pattern you’re dealing with.
IBS Subtype Comparison Key Takeaways
- IBS subtypes are IBS-C, IBS-D, IBS-M, and IBS-U.
- Rome IV uses recurrent abdominal pain plus stool pattern.
- Stool form and frequency help define each subtype.
- The Bristol Stool Scale supports clearer subtype tracking.
- A stool diary is more reliable than memory.
- Treatment should match the dominant bowel pattern.
- Worsening, persistent, or unclear symptoms need clinician review.
What Are the IBS Subtypes and How Do They Compare?

Irritable bowel syndrome is commonly divided into four subtypes in the Rome IV framework: IBS-C, IBS-D, IBS-M, and IBS-U (source). Clinicians sort them by stool form, bowel movement frequency, and your symptom history. That classification matters because it points treatment toward the pattern you actually have, not just the diagnosis name. A guide to IBS types can help you compare the basics.
All four IBS subtypes share one core feature. IBS usually means recurrent abdominal pain or discomfort that relates to bowel movements. Bloating, urgency, straining, and a feeling of incomplete emptying are also common. The stool pattern changes, but the pain-and-bowel link is what defines Irritable Bowel Syndrome.
Here is a simple side-by-side view:
| Subtype | Main stool pattern | Bristol Stool Scale | Common clues |
|---|---|---|---|
| IBS-C | Constipation-predominant IBS | Types 1 to 2 | Hard or lumpy stools, infrequent bowel movements, straining, a constant sense of constipation |
| IBS-D | Diarrhea-predominant IBS | Types 6 to 7 | Loose or watery stools, more frequent bowel movements, urgency, cramping, bathroom anxiety |
| IBS-M | Mixed IBS | Alternates between constipation-type and diarrhea-type stools | Both patterns show up at different times |
| IBS-U | Unclassified IBS | Does not clearly fit the other groups | Symptoms do not meet the usual subtype thresholds |
IBS-C is the constipation-heavy pattern. Stools are often hard, dry, and difficult to pass. Bloating and straining can make bowel movements feel unfinished. Bristol Stool Scale Types 1 and 2 often match this pattern.
IBS-D with diarrhea looks very different. Loose or watery stools are common, and the urge to get to a bathroom can hit quickly. Cramping often comes with it. If diarrhea is your main issue, managing IBS-D symptoms can become a practical part of daily planning.
IBS-M and IBS-U are less straightforward. IBS-M means your stool pattern flips between constipation and diarrhea. IBS-U is used when symptoms do not clearly meet the other subtype categories. In practice, that often means the symptoms are real, but the pattern does not fall neatly into one box under the usual 25% rule.
Subtype matters because treatment choices are not the same for every pattern. A constipation-prone pattern may lead to fiber changes, fluids, and constipation-focused medicines. A diarrhea-prone pattern may call for different food choices, antidiarrheal options, or other symptom control. Mixed or unclear symptoms make tracking even more important.
Before your next clinician visit, focus on these details:
- Stool form: Use the Bristol Stool Scale to note hard, loose, or mixed stools.
- Frequency: Track how often you have bowel movements each week.
- Pain timing: Notice whether pain improves or worsens after a bowel movement.
- Triggers: Write down foods, stress, travel, and sleep changes that seem linked to symptoms.
- Pattern over time: Watch for stretches of constipation, diarrhea, or alternating stools.
That record can clarify your IBS subtype and make treatment talks more useful. It also helps you and your clinician decide what to change first and what to monitor next.
How Do Rome III And Rome IV Differ?
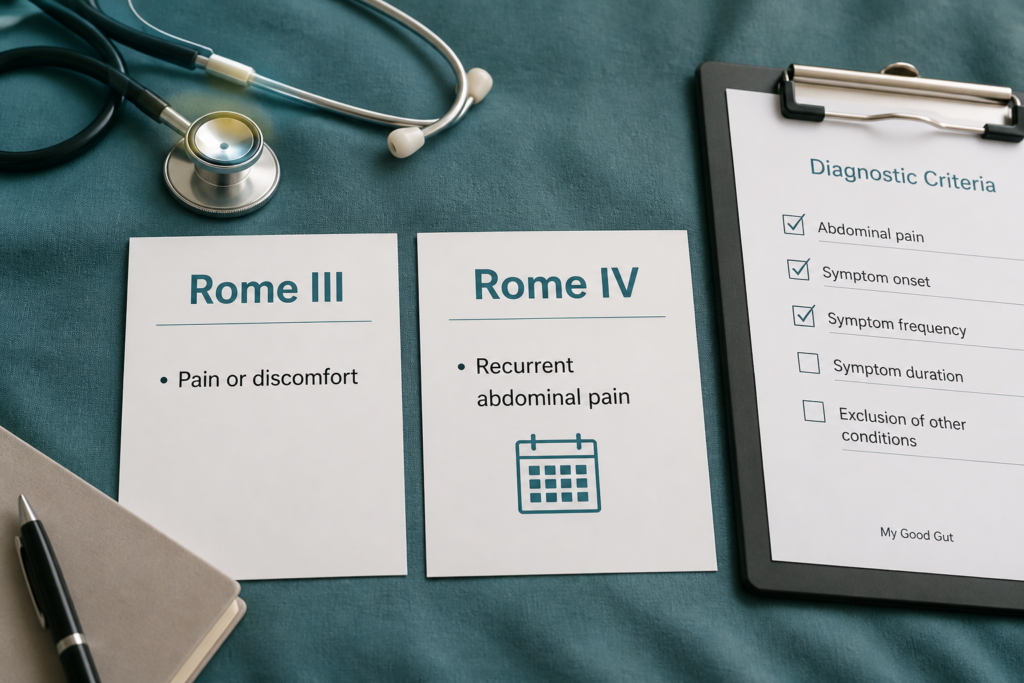
Rome IV criteria made the diagnosis of IBS more specific than the Rome III criteria. The biggest change was the pain rule. Rome III allowed abdominal pain or discomfort, while Rome IV requires recurrent abdominal pain (source). Rome IV is more specific, which can help clinicians apply the criteria more consistently and can reduce overlap with other digestive disorders (source).
Subtype labels depend on stool form, not only how often you go. Clinicians use the Bristol Stool Scale and the 25% rule to sort patterns into the main IBS subtypes:
| Subtype | Stool pattern |
|---|---|
| IBS-C | Hard or lumpy stools make up at least 25% of abnormal bowel movements, and loose or watery stools stay under 25% |
| IBS-D | Loose or watery stools make up at least 25% of abnormal bowel movements, and hard stools stay under 25% |
| IBS-M | Hard or lumpy stools and loose or watery stools both reach at least 25% |
| IBS-U | Symptoms do not fit the thresholds for the other subtypes |
That system works better when you track symptoms over time. Memory can be unreliable, especially if your pattern changes from week to week. A symptom diary can be more reliable than memory because recall over months may not match daily records, so shorter structured tracking can help clarify bowel patterns (source). A stool log gives a clearer picture than guessing from memory alone.
Tracking also helps when your pattern shifts. Stress, diet changes, and microbiome changes can move your symptoms in either direction. Loose stools can also come from other causes, including bile acid diarrhea, which may look like IBS-D at first. For that reason, subtype labels are best treated as a snapshot of your current bowel habits, not a permanent identity.
The practical difference between the two systems looks like this:
| Feature | Rome III | Rome IV |
|---|---|---|
| Core pain criterion | Abdominal pain or discomfort | Recurrent abdominal pain |
| Threshold style | Broader and less specific | Tighter and more specific |
| Subtype sorting | Stool pattern based | Stool pattern based with the Bristol Stool Scale and 25% rule |
For you, the main takeaway is simple. Rome IV asks about both pain and stool form because both shape the subtype and the next treatment step. If your symptoms are borderline or still changing, you may be classified as IBS-U first and reclassified after more tracking. That is a normal part of the process when sleep, stress, food triggers, or the microbiome change your pattern.
How Do You Classify Your Subtype With Stool Tracking?
A stool diary gives you the clearest way to sort out your IBS subtype because it tracks patterns over time instead of relying on one rough day. A simple poop diary for several weeks can show whether your stool pattern is mostly hard, loose, mixed, or fairly stable. It also helps you connect bowel changes with meals, stress, travel, illness, or medicine changes.
Start by logging every bowel movement with the date, time, and stool consistency using the Bristol Stool Scale. That scale runs from Type 1 to Type 7, and it gives you a shared language for describing what you see in the toilet. The goal is not perfection. The goal is a repeatable record that makes the diagnosis of IBS easier to discuss with a clinician.
Plain-language mapping can help you read the pattern faster:
| Bristol Stool Scale type | Common IBS pattern |
|---|---|
| Types 1 to 2 | Constipation-predominant symptoms |
| Types 3 to 4 | Middle range or more stable stools |
| Types 6 to 7 | Diarrhea-predominant symptoms |
Types 1 and 2 usually fit constipation-predominant IBS. Types 6 and 7 usually fit diarrhea-predominant IBS. Types 3 and 4 often sit in the middle, and they can help show when your symptoms are not clearly one extreme.
The Rome IV criteria classify IBS subtypes by the proportion of abnormal bowel movements in each stool pattern. IBS-C and IBS-D are assigned when at least 25% of abnormal bowel movements fit one pattern and fewer than 25% fit the opposite pattern (source). That rule matters because one bad flare should not define your whole picture.
A simple workflow can keep the log useful:
- Record each bowel movement right away.
- Mark the Bristol type for that stool.
- Note triggers that may matter, such as stress, diet changes, infection, or a new medicine.
- Review the full diary after several weeks.
- Count which abnormal stools show up most often.
That longer view matters because memory can be misleading. A 4-week daily log often lines up better than a 3-month recall, but the diary still gives more reliable detail than trying to remember your “usual” stools later. Your subtype should come from the full record, not from the worst day in a flare.
Mixed or shifting patterns need extra care. Mixed IBS can look like constipation on some days and diarrhea on others, so the diary helps you see which pattern reaches the threshold and which one stays below it. That is especially useful when symptoms shift with food changes, stress, infection, or treatment.
The subtype you identify should guide your next step with a clinician, because the wrong approach can worsen symptoms. A strong pro-motility plan during an unrecognized diarrhea phase may make loose stools worse. If your pattern changes over time, update the log and revisit the classification.
A good IBS tracking habit usually includes these basics:
- Date and time: When the bowel movement happened
- Stool type: Bristol type 1 through 7
- Related details: Pain, urgency, bloating, meals, stress, or medicine changes
- Pattern review: Which type appears most often across the full diary
This kind of tracking makes your symptoms easier to explain and your care easier to personalize. Digestive symptoms can have many causes, so persistent, severe, or worsening changes deserve medical review.
How Long Should You Track Symptoms?
Tracking symptoms for several weeks can provide a clearer picture than relying on memory alone, and a daily stool diary is a practical starting point for many people (source). A daily stool diary, or poop diary, helps you note stool form, urgency, constipation, and diarrhea as they happen.
A several-week log also helps balance two common problems:
- Too short: A few days can miss normal day-to-day swings.
- Too long: Recalling months of symptoms raises recall bias.
- More useful: About 4 weeks gives you a current snapshot of your IBS subtype.
That matters because IBS can shift over time. Stress, diet changes, sleep loss, and changes in the gut microbiome can all affect your pattern over weeks or months. Daily symptom tracking can be more dependable than long-term recall for classifying IBS patterns, so a structured diary is a useful way to review symptoms over time (source).
Recheck sooner if your pattern changes during or after the diary period. The point is to identify your present subtype and guide next steps, not to lock you into a label forever.
How Do You Count Borderline Days?
The Rome IV 25% rule is based on the share of abnormal bowel movements that match each stool form, not on the number of bad days in a calendar week (source). With the Bristol Stool Scale?? cannot invent links. No links provided, so plain text only. Need no markdown link. Let’s write with plain text. Need keyword Bristol Stool Scale exact. 2nd person okay.
Need maybe no links at all. final text with table and bullets. Let’s ensure table and concise. Need no heading repetition. Use “stool consistency”. Let’s draft with 190 words.
What Should You Do For Each Subtype?
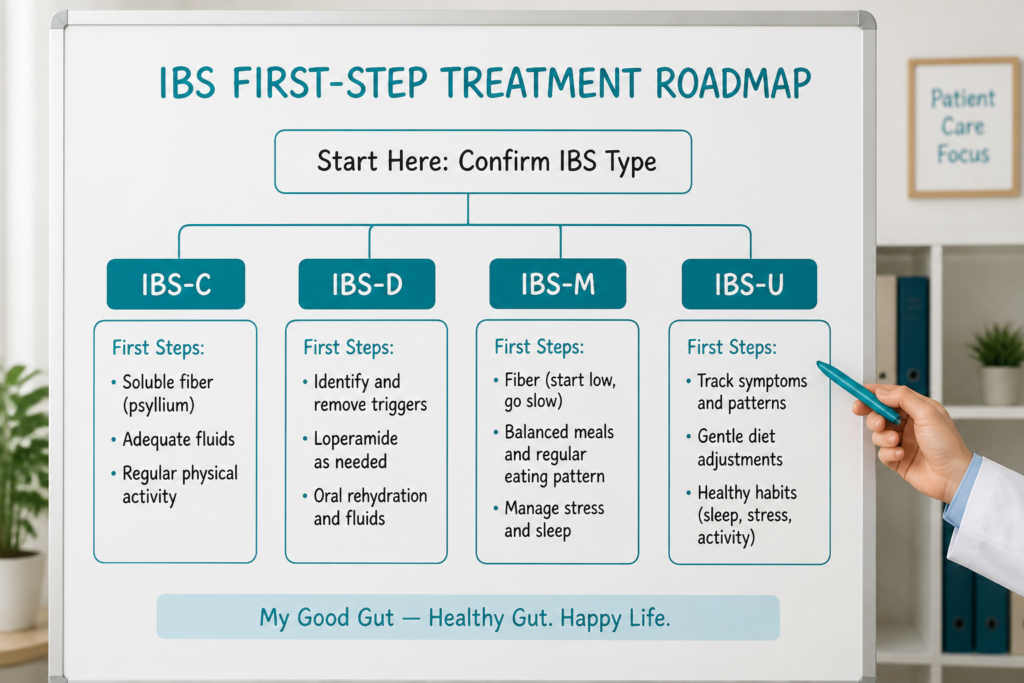
The safest approach is management by subtype. Start with the bowel pattern that is present now, then adjust treatment if symptoms stay disruptive or the pattern changes (source). That keeps treatment practical and helps you avoid chasing the wrong fix for too long.
A simple roadmap looks like this:
| Subtype | Start first | If symptoms persist | When to escalate |
|---|---|---|---|
| IBS-C | Soluble fiber, fluids, gentle movement | Osmotic laxatives, pro-motility agents, then secretagogues | Severe constipation, worsening pain, or alarm symptoms |
| IBS-D | Trigger reduction, a short low-FODMAP diet trial, less caffeine, less roughage | Loperamide, then selected bile acid treatments or rifaximin | Frequent diarrhea, dehydration risk, blood, fever, or nighttime symptoms |
| IBS-M | Treat the dominant pattern, not the label | Switch tools as the stool pattern changes | Ongoing swings, unclear pattern, or new red flags |
| IBS-U | Treat the main symptom cluster and keep tracking | Reassess after enough time for a clearer pattern to show | Persistent symptoms or signs that another condition may be present |
Constipation-Predominant IBS, or IBS-C, usually responds best to gentle bowel-support steps first. Soluble fiber such as psyllium can help stools hold water and move more easily. Adequate hydration and gentle movement also matter because both can support regularity without adding much risk.
If your IBS-C symptoms include hard stools, straining, bloating, or a feeling of incomplete emptying, that pattern points more toward IBS-C than ordinary constipation. Stool-softening strategies usually come before stronger medicines. For IBS-C, osmotic laxatives or prescription agents that increase intestinal fluid or movement may be used when fiber and fluids are not enough (source).
Some people need prescription help when constipation stays stubborn. Secretagogues such as linaclotide can be part of later treatment when bowel movements remain too infrequent or too difficult. Gut-directed therapies like hypnotherapy may also help some people with pain and bowel distress, but they should support care, not replace a medical check when constipation is severe, getting worse, or paired with alarm signs.
Diarrhea-Predominant IBS, or IBS-D, often improves most when you first remove obvious triggers. Caffeine, greasy meals, large portions, alcohol, and very rough foods can all make symptoms move faster. A short low-FODMAP diet trial can also help some people, especially when symptoms flare after certain carbs, but it works best as a guided, time-limited trial rather than a forever plan.
Medication for IBS-D usually comes after diet and trigger work. For IBS-D, loperamide can help reduce stool frequency and urgency, especially for short-term symptom control (source). If diarrhea stays frequent, your clinician may discuss bile acid sequestrants or rifaximin in selected cases, depending on your symptom pattern and history.
Bile acid diarrhea is worth considering when diarrhea keeps showing up despite simple changes. Some stool tests and blood tests can help look for it. That matters because not every IBS-D pattern is driven by the same cause. If your stools are loose often, especially after meals, a broader check can keep you from treating the wrong problem for months.
IBS-M is best handled as a flexible plan, not a fixed label. When constipation is the main problem, use constipation tools. When diarrhea takes over, shift to diarrhea tools. When pain or cramping is the biggest issue, antispasmodics may help more than bowel-focused medicine alone.
That kind of matching matters because mixed symptoms can swing in both directions. Treating the current bowel pattern helps avoid making constipation worse with diarrhea-focused choices or making diarrhea worse with constipation-focused ones. The goal is to follow the day-to-day pattern, not just the code in your chart.
IBS-U is a real category, not a dead end. It means your symptoms do not cleanly fit IBS-C, IBS-D, or IBS-M yet. That can happen when the pattern is still changing, when symptoms are not classic, or when stool history has not been tracked long enough to show a clearer direction. Under Rome III and Rome IV, the classification rules differ, so some people end up in IBS-U even when their symptoms are very real.
A few practical next steps can make this easier to manage:
- Track stools daily: Use the Bristol stool scale, bowel frequency, urgency, pain, and bloating.
- Match treatment to the dominant pattern: Use constipation tools on constipation days and diarrhea tools on diarrhea days.
- Keep trials short and focused: Try one change at a time so you can tell what helps.
- Watch for pattern shifts: New symptoms may mean your subtype needs to be reclassified.
The same escalation rule applies to every subtype. If first-line steps do not help, if symptoms get worse, or if red flags appear, it is time to talk with a clinician about testing and a broader workup. That includes weight loss, bleeding, fever, anemia, and nighttime symptoms that wake you up or keep you from sleeping.
Persistent or severe symptoms deserve a closer look, even if they seem to fit IBS at first. Digestive symptoms can have many causes, and a broader evaluation can help rule out conditions that need different care. Staying open to reclassification is part of good IBS care, because the best plan is the one that matches the pattern you actually have now.
For most people, the best care path is calm and stepwise. Start with the subtype that fits your current symptoms, use the mildest effective tools first, and escalate when the picture stays unclear or the symptoms stop being manageable. That approach supports your gut health without overreacting, and it gives you a clearer route to the next right test or treatment.
IBS Subtype FAQs
These FAQs cover the most common questions about IBS subtypes so you can make sense of symptom patterns, triggers, and treatment choices without guesswork.
They also explain how subtype differences can shape your daily comfort and quality of life.
1. Can IBS Subtype Change Over Time?
Yes, your IBS subtype can change with stress, diet shifts, and changes in the microbiome. Stress, diet shifts, and changes in the microbiome can make your symptoms look more like IBS-C, IBS-D, IBS-M, or IBS-U from week to week or month to month. Subtype is only part of the picture, since abdominal pain and discomfort can make IBS feel severe even when your stool pattern stays similar. If your bowel habits change often, stool tracking can help you and your clinician tell temporary variation from a longer-term subtype shift.
2. What Is IBS-Mixed?
Mixed IBS means your stools swing between constipation and diarrhea, with hard or lumpy stools and loose or watery stools each present in at least 25% of bowel movements. One stretch may bring straining, infrequent stools, or a feeling of incomplete emptying, while another brings urgency and loose stools, and bloating or abdominal discomfort can show up in both. Possible explanations include overflow from severe constipation and an unstable gut–brain interaction that affects motility, so symptom tracking helps you match diet, stool-regulating strategies, or antispasmodics to your current pattern and discuss lasting changes with a clinician.
3. How Accurate Is Stool-Based Classification?
Stool-based classification uses the Rome IV 25% cutoff, so a subtype is identified when at least 25% of abnormal bowel movements match one pattern and less than 25% match the opposite one. A daily stool diary with the Bristol Stool Scale is usually more accurate than memory because it captures day-to-day changes in real time, while recall-based subtyping is only moderately consistent with diary data. One study found that 88% of people with IBS-C remembered more hard-stool days than loose-stool days over 3 months. Because IBS subtypes can shift with stress, diet, abdominal pain severity, and visceral hypersensitivity, clinician review or objective testing is wise when symptoms are mixed, borderline, persistent, severe, or worsening.
4. When Should You Recheck Your Subtype?
IBS subtype can shift over time, sometimes within a few months, so it makes sense to recheck when treatment is not helping or your bowel pattern no longer matches the one you first tracked. Reassessment matters if treatment is not helping, or if a medicine for one pattern seems to make symptoms worse, such as a pro-motility approach during an unrecognized diarrhea phase. Recent antibiotics, an infection, a major diet change, or a big stress shift can also change symptoms enough to justify fresh stool tracking, and blood in the stool, weight loss, fever, or waking at night with severe symptoms should prompt medical evaluation.