IBS symptoms in children can look like ordinary stomach trouble, but the pattern often keeps returning and starts to affect meals, school, and family routines. Parents and caregivers often face the tension between wanting reassurance and needing to know when belly pain, bloating, constipation, or diarrhea points to something more than a passing bug. IBS is a functional gastrointestinal disorder, which means the digestive tract usually looks normal while how it works is disrupted. The goal is to sort out the symptom pattern, common triggers, and warning signs that need a pediatrician's attention.
The sections ahead cover the most common symptoms, how stool changes help distinguish IBS-C, IBS-D, and mixed patterns, and which foods and routines can set off flares. They also explain how clinicians use the Rome IV pediatric criteria, when tests such as blood work or stool studies may help, and why FODMAP foods sometimes matter. A symptom log, a red flag checklist, and practical next steps at home give families something concrete to use before the next appointment.
Parents, teachers, and other caregivers will find the most value here when a child keeps complaining of abdominal pain or bathroom urgency but still seems well between episodes. That matters because normal growth and normal scans can fit IBS, while blood in the stool, weight loss, fever, or nighttime pain call for a different path. For example, a child who has cramping after lunch, bloating after dairy, and constipation during stressful school weeks may be showing a repeatable pattern, not random upset. Keep reading for clear, clinician-reviewed guidance that helps turn uncertainty into a plan.
IBS Symptoms in Children Key Takeaways
- Recurrent abdominal pain is the hallmark IBS symptom in children.
- IBS may cause constipation, diarrhea, or alternating stool patterns.
- Bloating, gas, urgency, and mucus often cluster during flares.
- Normal tests and normal growth can still fit pediatric IBS.
- FODMAP foods, dairy, stress, and routine changes may trigger symptoms.
- Blood in stool, weight loss, fever, or nighttime pain need prompt evaluation.
- A symptom log helps pediatricians spot patterns and guide next steps.
What Is IBS In Children?
Irritable Bowel Syndrome in children is a common, long-lasting digestive condition that often starts in childhood or the teen years. It can affect comfort, meals, school attendance, sports, sleep, and the daily rhythm of family life. The symptoms are real even when tests do not show damage.
IBS in children is a functional gastrointestinal disorder. That means the digestive tract usually looks normal on exams and scans, but it does not work in the usual way. The pain is not imaginary. The problem is how the system functions, not obvious injury such as inflammation, ulcers, or tissue breakdown.
The gut and brain communicate constantly. In pediatric IBS, that signaling can become overly sensitive, almost like the volume has been turned up too high. That can lead to:
- Belly pain or cramping
- Diarrhea, constipation, or both
- Bloating and gas
- Stool changes that seem to come and go
- Symptoms that flare after meals, stress, or routine changes
Normal test results can fit this diagnosis. When blood work, stool tests, or other checks do not show inflammation or structural disease, that can support pediatric IBS rather than rule it out. The goal is to match the symptom pattern with the right diagnosis, not to chase every test result in isolation.
Pediatric IBS does not cause permanent structural damage to the digestive tract. That helps separate it from diseases that scar or injure the intestines over time. A child may still feel miserable, miss class, or avoid food because of fear of pain, but the bowel itself is usually not being physically destroyed.
The condition is also more common than many parents expect. Estimates suggest that Irritable Bowel Syndrome in children affects a significant portion of kids, with some studies reporting rates between 6% and 14%, and higher prevalence in girls compared to boys (source). That makes IBS in children a familiar pattern for pediatric clinicians, even when it feels confusing at home.
What families should know | Why it matters |
|---|---|
Common in childhood | It is a familiar pattern for pediatric clinicians |
Functional, not structural | Symptoms can be severe even when tests look normal |
Linked to gut-brain signaling | Stress, meals, and bowel habits can affect symptoms |
Usually not damaging | Normal growth and exams can still fit IBS |
Because this is a functional disorder, the first step is usually to focus on symptoms, triggers, and red flags instead of assuming a child needs a large workup right away. That approach helps pediatricians decide when careful monitoring is enough and when more testing is needed.
What Symptoms Are Most Common?
Recurrent abdominal pain is the hallmark pattern in irritable bowel syndrome (IBS) in children, and it overlaps with the overall IBS symptoms seen at any age. The pain often lasts longer than 3 months, typically occurring around the belly button or lower abdomen, and may come and go rather than staying steady all day (source). It can ease or flare around bowel movements, which is why common IBS symptoms often show up as a pattern rather than one isolated complaint.
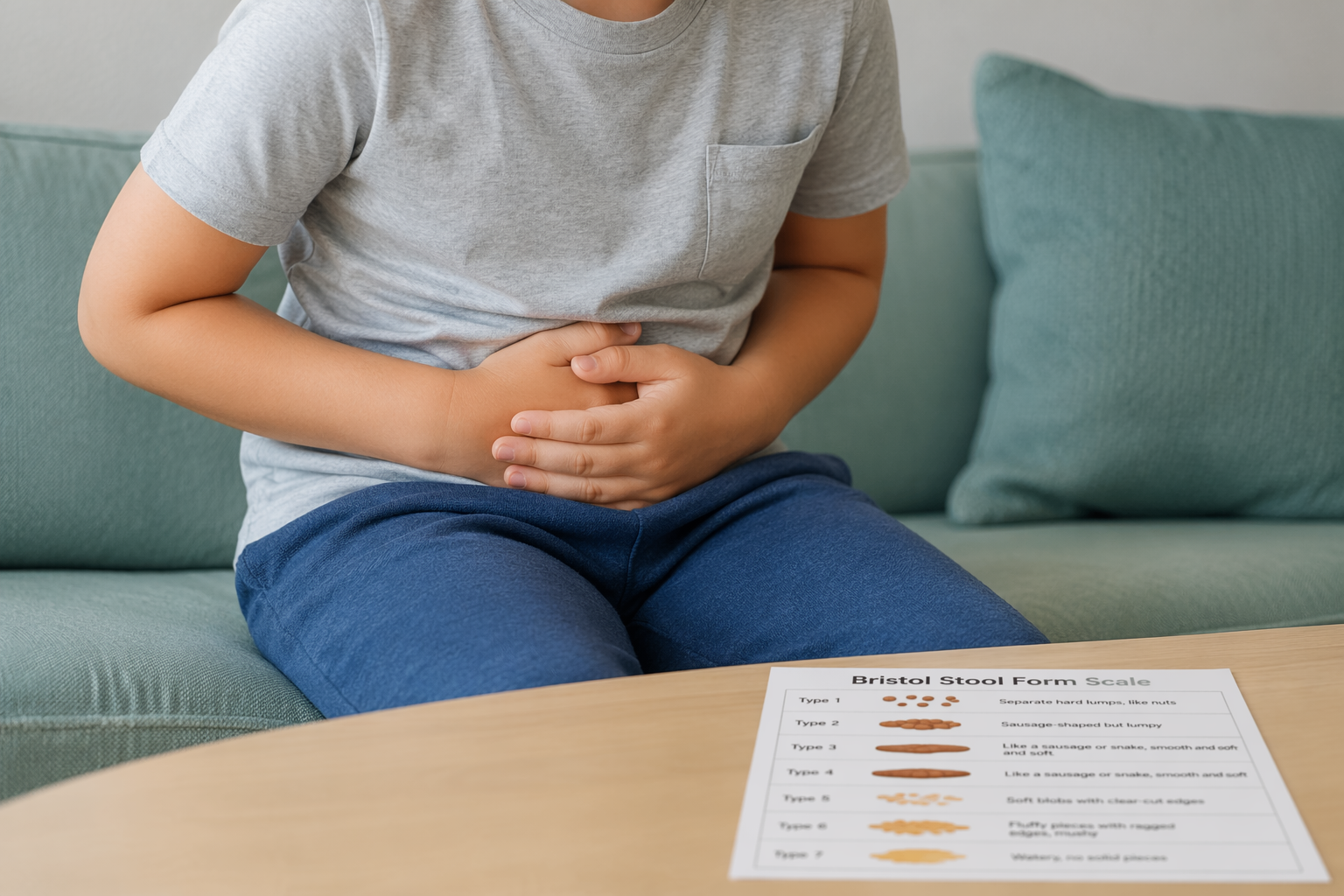
The stool pattern helps sort out the main IBS types. Some children have hard, painful stools and go less often, which points to constipation in children, or IBS-C. Others have diarrhea in children with loose or watery stools and a sudden need to go, which fits IBS-D. A third group has alternating diarrhea and constipation, often called IBS-M. Pediatric clinicians often look at stool shape and timing over time, including the Bristol Stool Form Scale, to see which pattern fits best.
A few symptoms tend to cluster around the bathroom itself:
- Urgency: A child feels like they need to go right away, and IBS urgency can be stressful at school or during activities.
- Incomplete evacuation: A child still feels like there is more to pass after using the toilet.
- Mucus in the stool: Small amounts of mucus can appear during flares.
These symptoms usually flare on and off, not every single day without change.
Bloating, abdominal fullness, and extra gas are also very common. A child may say the belly feels tight, swollen, or uncomfortable after meals or later in the day, even if it does not look visibly distended. That kind of bloating and gas children notice can be easy to miss at first because the discomfort is often more obvious than the swelling.
IBS in children usually shows up as a cluster of symptoms, not just one sign in isolation. The mix often includes pain, stool changes, bloating, bathroom urgency, and sometimes mucus. Some children also seem tired, uncomfortable, or distracted during flares. A short stomach bug usually passes faster, while IBS symptoms tend to recur over weeks or months and track with bowel habits.
Pattern | More suggestive of IBS | More suggestive of a short infection |
|---|---|---|
Pain | Recurrent abdominal pain that keeps returning | New pain that settles within a few days |
Stool changes | Ongoing constipation, diarrhea, or switching between both | Brief diarrhea or constipation that resolves |
Other clues | Bloating, urgency, mucus, and incomplete emptying | Fever, vomiting, or a clear sick-day pattern |
Mild daytime fatigue can happen with a flare, but IBS should not cause severe, worsening, or progressive warning signs. Persistent or intense symptoms still need medical evaluation, especially if the pattern feels different from the usual abdominal pain in children you've seen before.
How Can You Tell IBS From Other Conditions?
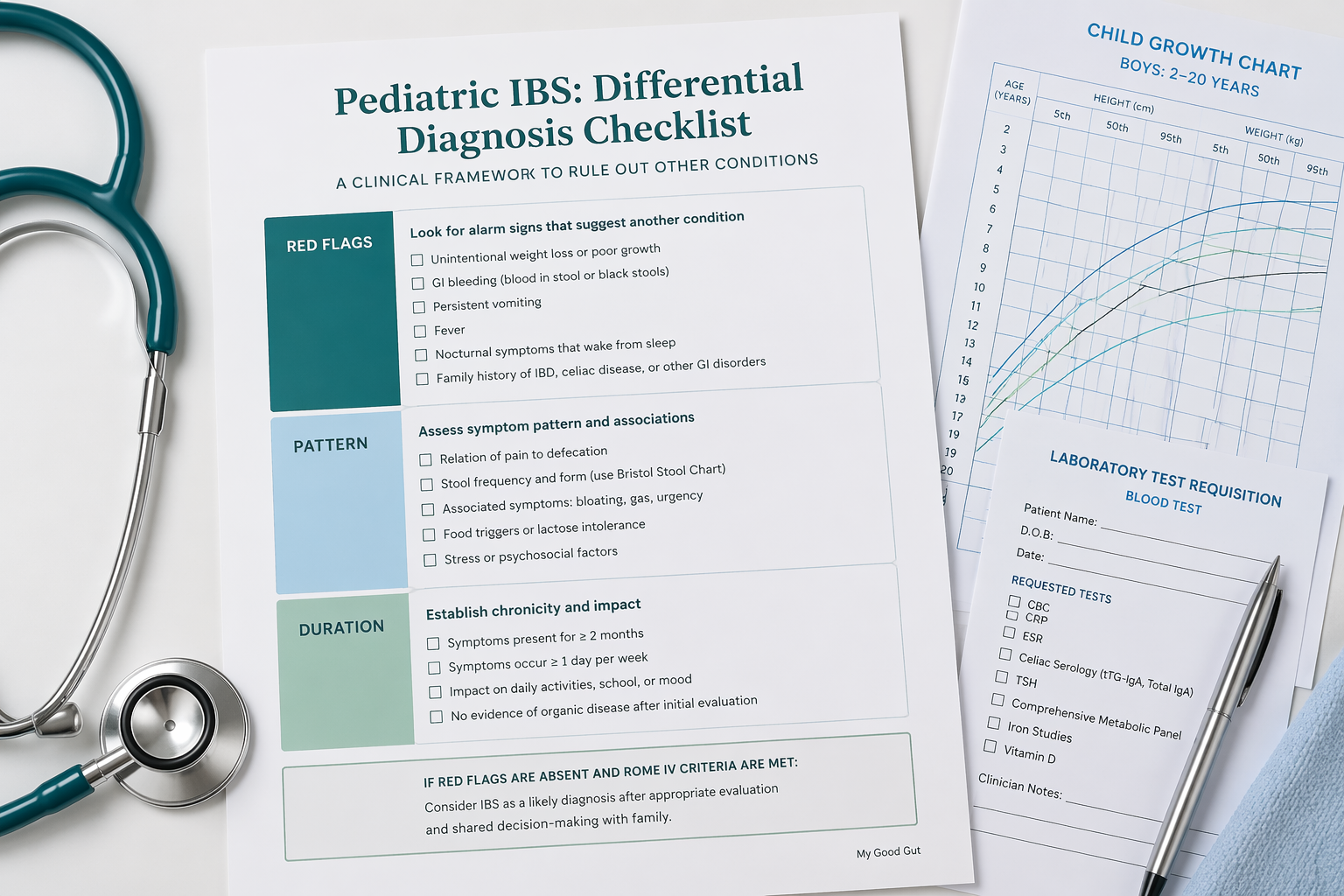
IBS in children usually does not show up on a single test. Clinicians build the picture from your child's symptom pattern, a physical exam, and selective testing that rules out other causes. The Rome IV pediatric criteria help doctors decide whether the pattern fits IBS, requiring pain at least 4 days a month for 2 months or longer, along with changes in stool form or frequency (source, source).
The details that matter most are simple but important:
- Age and timing: when symptoms started and how long they have been going on
- Pattern: whether belly pain or bowel changes come and go in a repeated cycle
- Warning signs: whether there is blood, fever, or weight loss in children
- Sleep disruption: whether pain or diarrhea wakes your child at night
A child who keeps normal growth, has no fever, and has no blood in the stool is more likely to have IBS than a child with bloody diarrhea child or another red-flag pattern. Those red flag symptoms children should shift the workup away from IBS and toward prompt evaluation. The same is true with poor growth or delayed puberty, persistent or severe vomiting, severe dehydration, pain in the upper right or lower right abdomen, joint pain, or unexplained skin rashes.
When IBS is not the only possibility, clinicians may order targeted diagnostic tests pediatric IBS rather than broad screening. Those tests often include:
- Blood work: to look for anemia, inflammation, celiac disease, or other clues
- Urine testing: to help rule out urinary causes of pain
- Stool studies: including stool tests occult blood and checks for infection
- Other labs: to look for inflammatory bowel disease, food intolerance, or structural problems
Additional testing depends on the symptoms and exam findings. A child with bloating, gas, or loose stools may need a lactose breath test if lactose intolerance child seems likely. Breath tests can also help assess sugar malabsorption or SIBO. If the picture still does not fit, a clinician may suggest an abdominal X-ray, ultrasound, and, more rarely, endoscopy or colonoscopy.
A typical IBS pattern still carries weight. Normal growth, no blood, no fever, and symptoms that follow a familiar pattern make IBS more likely. Even so, persistent or worsening pain or bowel changes over several weeks deserve follow-up so your pediatrician can reassess and decide whether more testing is needed.
What Triggers Pediatric IBS Flares?

IBS flares in children often follow a pattern, not one single bad day. You may notice belly pain, bloating, constipation, diarrhea, or urgency after a certain meal, a stressful school day, or a routine that got thrown off. Watching for repeating patterns is more useful than blaming the last thing your child ate.
Common triggers often come from FODMAP foods, which include onions, garlic, apples, wheat, milk, honey, and legumes, as these can increase gas and pull water into the gut (source, source). In some children, these foods pull extra water into the gut and make more gas, which can worsen cramping and bloating and gas children experience.
Other meals can matter just as much. Dairy, large meals, fast food, spicy dishes, and high-fat meals may be harder to digest or may slow stomach emptying. That is why symptoms often show up after a heavy lunch, a restaurant dinner, or eating too quickly between activities.
Stress can be a real trigger too. Stress and anxiety in pediatric IBS can make the brain and gut react more strongly together. School anxiety, home stress, tests, social pressure, or worry about symptoms can turn mild discomfort into a stronger flare, even when no clear food trigger is present.
Routine changes can set off symptoms as well. Travel, sleep schedule shifts, skipped meals, sports weekends, holidays, and changes in bathroom timing can disrupt regular eating, rest, and movement. Those changes may worsen constipation, diarrhea, or cramping because the gut tends to do best with a steady rhythm.
Common flare links to watch for:
- Meals: onions, garlic, wheat, milk, apples, honey, beans, or lentils
- Heavy eating: large portions, fried food, fast food, or rich restaurant meals
- Stress: school pressure, family tension, tests, or social worries
- Routine shifts: travel, late nights, skipped breakfast, or delayed bathroom breaks
Sometimes symptoms also flare when another gut issue is present, such as bacterial overgrowth or changes in the gut microbiome and IBS pattern. A breath test SIBO may be part of a doctor's workup when symptoms point in that direction. Probiotics children take may help some kids, but they should not replace medical evaluation or a plan that fits your child's needs.
The most useful next step is a simple symptom log with meals, stress, sleep, and bathroom habits. That record can help you and your pediatrician spot patterns and decide whether a low FODMAP diet children can try, or whether another cause needs to be checked first. This content is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, so you should consult a qualified healthcare professional for persistent, severe, or worsening symptoms. Results vary by person, and any dietary or supplement advice should be individualized.
What Should You Track And Do Next?

A simple log can make the pattern much clearer, and it can help your child’s clinician separate IBS from something else.
Write down these basics:
- Pain pattern: when it starts, where it hurts, how long it lasts, how often it happens, and whether it follows meals, school stress, travel, or a bowel movement
- Stool details: stool frequency, stool form, urgency, constipation, diarrhea in children, accidents, and whether the pain improves after pooping
- Context clues: your child’s age, how long the symptoms have lasted, and warning signs like blood in the stool, fever, nighttime pain, vomiting, or weight loss in children
The Bristol Stool Form Scale can help you describe stool shape more clearly. Several days of notes are more useful than one rough day because repeated patterns matter more than a single flare.
The next step is to look for triggers without treating every stomachache like an emergency. Pain after a large meal, bloating after dairy, gas or urgency after FODMAP-heavy foods, and worse symptoms during stressful school days can all point toward a pattern. That pattern helps guide what happens next.
Simple home steps often help with comfort and routine:
- Meal timing: keep meals and snacks more regular
- Hydration: offer steady fluids through the day
- Bathroom routine: build in a predictable time to sit on the toilet, often after meals
- Movement: encourage age-appropriate physical activity
- Food changes: narrow the pattern first before making broad cuts, and keep any elimination or low-FODMAP trial individualized with a clinician or a pediatric dietitian
A careful red flag check matters more than watchful waiting when symptoms are changing. Call your child’s clinician now if you notice these red flag symptoms children should not ignore:
- Persistent or worsening pain
- New or major bowel habit changes
- Poor growth or weight loss in children
- Pain that wakes your child at night
- Blood in the stool
- Fever, repeated vomiting, dehydration, or a child who seems increasingly unwell
Pediatric gastroenterology referral makes sense when symptoms keep going, the diagnosis is still unclear, or the clinician needs to rule out lookalike conditions. That can include celiac disease, inflammatory bowel disease, constipation, lactose intolerance, or infection. Diagnostic tests pediatric IBS may include stool tests occult blood, blood work, or other targeted testing, depending on the story.
The goal is not to label every symptom. It is to track enough detail to spot patterns, act early on red flags, and get the right help when your child needs it.
IBS Symptoms in Children FAQs
These FAQs cover common concerns about Irritable Bowel Syndrome in children, from belly pain and stool changes to signs that something else may be going on. They also help you compare patterns with IBS symptoms among women without overreading every ache or bathroom change.
1. What Foods Trigger IBS In Children?
Common triggers for IBS in children often include high FODMAP foods such as onions, apples, wheat, milk, and honey, which can vary from child to child. Milk and other dairy foods can also be a problem, especially if your child has a lactose intolerance child pattern, and large meals, fast food, and greasy foods may make symptoms worse. Because triggers vary from child to child, it helps to track what your child eats along with pain, bloating, diarrhea, or constipation, then review the pattern with a pediatric dietitian instead of using a long-term food restriction plan or a strict FODMAP foods list on your own.
2. How Is IBS In Children Treated?
Treatment for pediatric IBS is individualized because your child’s age, symptoms, and food tolerance shape the plan. Care often starts with diet changes such as a short low FODMAP diet children trial with a dietitian, lactose limits if needed, and soluble fiber for constipation in children or loose stools. A clinician may also suggest probiotics children, symptom medicines, and therapies that support stress and anxiety in pediatric IBS, such as CBT, hypnotherapy, relaxation, or guided imagery, but worsening symptoms or red flags should prompt a medical review.
3. How Long Do IBS Symptoms Last?
IBS in children usually follows a long-running pattern, not a one-day or two-day upset, and it tends to recur over weeks or months. Your child may have [recurrent abdominal pain] for more than 3 months, often near the belly button or lower abdomen, and it can fluctuate with bowel movements. Under the [Rome IV pediatric criteria], doctors look for pain at least 4 days a month for 2 months or longer, along with changes in stool form or frequency, such as [alternating diarrhea and constipation].
4. When Should You Call A Doctor?
Call your child’s doctor if belly pain keeps coming back, wakes them from sleep, or comes with bowel changes that are getting worse, especially if the pattern changes. Seek prompt evaluation for bloody stools, bloody diarrhea child, black stools, unexplained weight loss, poor growth, delayed puberty, or a swollen liver, since these findings need assessment. Get urgent care for severe dehydration, repeated vomiting, fever without a clear cause, nighttime diarrhea that disrupts sleep, or pain in the upper right or lower right belly, because these signs can point to something other than IBS.
