IBS urgency is the sudden need to reach a bathroom fast, and it can turn ordinary routines into a constant planning exercise. For adults living with IBS, the hard part is often not just loose stool but the fear that there won’t be enough time to wait, drive, or finish a meeting. In plain terms, urgency means the bowel signal feels immediate and difficult to delay, and the next step is knowing what sets it off, what helps, and when it needs medical attention.
That picture usually includes more than one factor, from rapid transit and a strong gastrocolic reflex to stress and rectal sensitivity. This article covers the most common causes, practical relief strategies, food and fiber changes, pelvic floor support, and the red flags that point beyond IBS. It also gives a simple framework for tracking patterns so a dietitian or clinician can use the details instead of guessing.
That matters most for people managing IBS around work, caregiving, travel, or long commutes, especially when urgency has started to shape daily decisions. A person who notices worse symptoms after breakfast, for example, may find that smaller meals, soluble fiber, and a bathroom plan make the day more predictable. My Good Gut keeps the focus on clear next steps so readers can move from uncertainty to a more workable routine.
IBS Urgency Key Takeaways
- IBS urgency is a sudden, hard-to-delay need to use the bathroom.
- It can happen with mild loose stool, cramping, bloating, or abdominal pain.
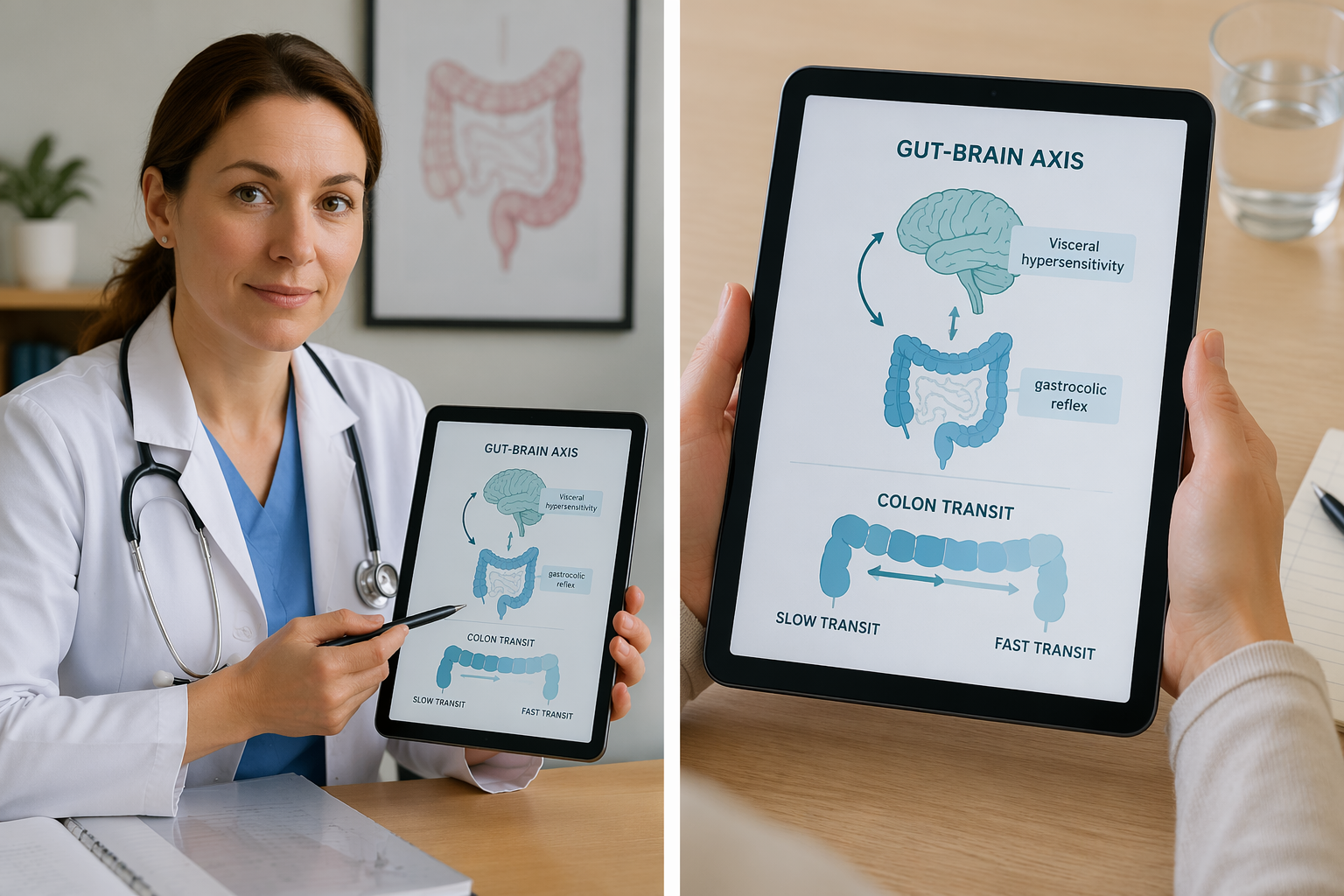
- Rapid transit, visceral hypersensitivity, and the gastrocolic reflex can drive urgency.
- Stress can intensify urgency through the gut-brain axis.
- A stool diary helps spot meal, stress, and timing patterns.
- Soluble fiber, smaller meals, and a low-FODMAP trial may help.
- Blood, fever, weight loss, or nighttime diarrhea need medical review.
What Is IBS Urgency?
IBS urgency is a sudden, hard-to-ignore need to get to a toilet fast. The urge can feel so strong that you only have a few minutes before an accident becomes a real risk. For some people with IBS, urgency can become a frequent part of the daily symptom pattern. Patient-facing guidance and clinical reviews describe urgency as a common and burdensome IBS symptom, but the exact share of adults affected varies by study and population (source, source).
Bowel urgency is not the same as loose stool alone. It can happen even when stool is only mildly loose, and it often shows up with cramping, bloating, or abdominal pain. IBS symptom patterns often start with this kind of unpredictable gut pressure. That is why the symptom can feel so disruptive.
The difference from a routine bowel urge usually comes down to how fast it hits, how much pressure it creates, and how hard it is to delay. The feeling can be especially stressful because you may not trust your body to wait.
Common signs of IBS urgency include:
- Speed: it comes on quickly and leaves little time to plan
- Pressure: it feels stronger than an ordinary bathroom signal
- Stress: it can trigger worry about making it in time
- Delay: it is much harder to put off than a normal urge
This content is for educational purposes only and is not a substitute for personalized medical advice.
Why Does IBS Urgency Happen?
IBS urgency usually starts with a mismatch between what your gut senses and what your brain expects. It is often the result of several signals getting louder at once, not one single problem.
Visceral hypersensitivity is one big reason. The nerves in your gut overreact to normal stretching. A small amount of gas or stool can feel painful or urgent, even when the bowel is not very full. That is why a mild shift in pressure can feel like an emergency.
Timing matters too. In IBS, stool may move too fast through the colon. That pattern is called rapid transit, and it affects colonic transit more broadly. When stool reaches the rectum before enough water is absorbed, urgency can hit fast and hard.
The gastrocolic reflex also plays a role. This is the normal after-meal signal that tells the colon to make room for food. In IBS, that response can be exaggerated. Many people notice that urgency is worse soon after meals, and the gastrocolic reflex can feel more noticeable after breakfast in some people with IBS (source, source).
Stress can turn the volume up through the gut-brain axis. Anxiety, fear of an accident, and constant symptom checking can keep your nervous system on alert. That can amplify gut signals and make urgency feel harder to control. In some people, calming the bowel also helps IBS gas relief.
A few parts of the system help explain why it feels so sudden:
- Rectal fill: stool reaches the end of the bowel quickly
- Stretch response: the rectum reacts strongly to small changes
- Alarm threshold: the brain reads the signal as urgent
Rectal compliance matters here too. When the rectum does not stretch as well, even a modest amount of stool can trigger a strong need to go. IBS urgency usually reflects how the gut and nervous system communicate, and different people may have different main triggers.
How Do You Tell IBS From Other Causes?
IBS urgency often follows a pattern. You may notice it in the morning, after meals, or during stress, and the stool pattern may swing between loose stools and constipation. Tracking stool consistency with the Bristol Stool Form Scale can help you spot that pattern. Sudden watery urgency without a longer history deserves a closer look.
The signs that point away from IBS are usually easier to spot:
- Inflammation clues: blood in the stool, black or tarry stools, unexplained weight loss, persistent fever, nighttime diarrhea, or symptoms that begin after age 50
- Infection clues: abrupt onset, fever, recent travel, sick contacts, or a short, intense bout of diarrhea
- Bile acid clues: watery, urgent stools, especially after gallbladder removal, which can fit bile acid malabsorption
- Medication clues: metformin, magnesium, antibiotics, laxatives, and other drugs that can trigger diarrhea and urgency
- Pelvic-floor clues: trouble holding stool, leakage even with formed stools, or a sense of incomplete emptying, which may reflect rectal compliance or muscle control problems
A stool diary can make these patterns easier to see. mucus during IBS flares can also help you sort out another symptom that often causes worry.
When the picture is unclear, clinicians may use simple tests to rule out other causes. Common options include blood work, celiac screening, inflammatory markers, and stool studies. If bile acid malabsorption seems likely, targeted testing or a trial of cholestyramine may be considered. Rapid transit and SIBO can also come up when symptoms do not fit a classic IBS pattern.
If urgency is severe, frequent, or hard to explain, ask for a basic workup or a gastroenterology referral. A dietitian can also help you match symptoms to the right food and treatment plan.
What Should You Do When Urgency Hits?

A quick reset can help when urgency hits in a store, car, or airport. The goal is not to force the feeling away. It’s to get yourself to the nearest bathroom with as much calm and control as possible.
Start with a five-minute calm-down sequence:
- Pause: Stop moving if it’s safe.
- Settle: Sit or stand still and relax your shoulders, belly, and jaw.
- Breathe: Take slow belly breaths through your nose and let your stomach rise on the inhale and fall on the exhale.
Deep diaphragmatic breathing can help calm the nervous system, and relaxation-based approaches may reduce stress-driven gut reactivity for some people. That can make urgency feel more manageable in the moment (source, source).
Breathing works even better with the Squeeze and Breathe method. Gently contract your pelvic floor for a few seconds, then release while keeping your breath steady. This is not a hard clench. It’s a brief reset that can help you feel more in control while you move toward the bathroom.
While you wait, keep your body relaxed and give your mind something else to do. These tactics can help:
- Count backward by 7s or 3s.
- Read signs, directions, or labels.
- Focus on a hard mental task.
- Hold a short conversation if it feels safe.
- Walk slowly instead of rushing.
Some people use an over-the-counter anti-diarrheal such as loperamide for predictable diarrhea-related urgency, including before travel or other high-stress situations, if a clinician or the product label says it is appropriate. Blood in the stool, fever, or symptoms that are unusual for that person should prompt medical review instead of self-treatment (source, source).
A same-day plan can lower panic before it starts. Map restrooms ahead of time, choose easier seats or routes when you can, and keep tissues, wipes, and any approved medicine in a small kit.
This rescue plan is a bridge, not a fix. If urgency keeps happening, ask a healthcare professional about diet changes, smaller meals, pelvic floor physical therapy, biofeedback for bowel, psychological therapies, or testing for other causes like infection, bile acid malabsorption, celiac disease, or inflammatory bowel disease.
How Can You Reduce IBS Urgency Day-To-Day?

A calmer gut routine can lower urgency, but it usually takes a few small changes rather than one big fix.
If urgency seems tied to meals, a low-FODMAP diet is one common first-step option to discuss with a registered dietitian or clinician. Guideline-based care also emphasizes finding personal triggers and adjusting diet in a structured way (source, source).
A food diary for IBS can help you spot meal patterns that guesswork misses. Tracking meals, symptoms, stool form, and timing for 1 to 2 weeks can give you a useful record to review with a clinician or dietitian (source, source).
Track these common triggers and note what happens after each meal:
- Dairy
- Caffeine
- High-fat or fried foods
- Alcohol
- Sugar alcohols like sorbitol and xylitol
Fiber can help, but the type matters. Soluble fiber, such as psyllium husk or oats, can absorb water and help firm loose stools. Insoluble fiber, like bran or raw vegetable skins, may move through too fast and worsen urgency for some people. Change your intake slowly and watch your stool pattern.
Meal habits matter more than many people expect. Large meals can trigger the gastrocolic reflex, which is the natural urge to poop after eating. Smaller meals, slower eating, and a calmer breakfast routine can reduce that post-meal rush.
Common day-to-day tools can be grouped like this:
Tool | What it may help with |
|---|---|
Low-FODMAP diet | Meal-related urgency, gas, loose stools |
Soluble fiber | Stool form and control |
Pelvic floor physical therapy | Holding back an urge long enough to get to the bathroom |
Relaxation and CBT | Stress-linked gut reactivity |
When urgency is frequent, pelvic floor physical therapy and biofeedback may help improve bowel control in some people. CBT for IBS is usually part of steady symptom management rather than an instant fix (source, source).
Your nervous system is part of the picture too. Diaphragmatic breathing, mindfulness, gut-directed hypnotherapy, and Cognitive-Behavioral Therapy can lower gut reactivity over time. CBT for IBS works best as steady support, not as an instant fix.
Test one change at a time for a short, set period. Keep track of stool form, timing, stress, meal size, and symptoms. Keep what helps, and get medical advice for persistent symptoms, worsening symptoms, or red flags. This content is educational only and is not a substitute for personalized medical advice.
When Should You See A Doctor?
IBS urgency deserves medical review when it stops feeling occasional and starts becoming a pattern. If it is frequent, severe, getting worse, or making work, travel, sleep, or daily routines hard to manage, it’s time to check in with a clinician. Stress can make symptoms louder through the gut-brain axis, but ongoing urgency should not be brushed off as just stress.
Certain red flags need prompt attention:
- Blood in the stool
- Black or tarry stools
- Unexplained weight loss
- Fever that keeps coming back
- Diarrhea that wakes you from sleep
- New bowel urgency that starts after age 50
Symptom details also matter because they help sort out Irritable Bowel Syndrome from other causes. A clinician will usually ask when urgency happens, whether it shows up after meals or in the morning, and whether it comes with diarrhea, constipation, or both. Stool consistency can be especially useful, since very loose stool raises the risk of accidents and may point to a different pattern than classic IBS.
Bring up urgency that does not improve after diet changes, over-the-counter products, or your usual self-care. Poor response can mean your plan needs to change, or that another condition should be ruled out. In some cases, targeted testing for inflammatory bowel disease or celiac disease may be the next step. A gastroenterologist or dietitian can then help match treatment to your stool pattern and triggers.
IBS Urgency FAQs
These FAQs cover the most common questions about IBS urgency and bowel urgency in everyday life. They also point you toward simple next steps and clear signs that medical care may be needed.
Stress, anxiety, and fear can make IBS urgency feel stronger because the gut and brain communicate through the gut-brain axis. Deep breathing may help with short-term calming, and CBT or gut-directed hypnotherapy may help some people manage symptoms over time (source, source).
An over-the-counter anti-diarrheal like loperamide can slow bowel movement and may help make stool less watery for some people with predictable diarrhea-related urgency. If cramping or gut spasms are part of the problem, antispasmodics or selected neuromodulators may be discussed with a clinician as part of IBS treatment (source, source).
1. Can IBS Urgency Happen Without Diarrhea?
Yes, IBS urgency can happen even when your stool is not very loose, and cramping, bloating, and abdominal pain can make that urge feel stronger. Cramping, bloating, and abdominal pain can make that urge feel stronger. When diarrhea is present, urgency is often seen with IBS-D, but urgency alone does not rule other IBS patterns in or out.
2. What Foods Trigger IBS Urgency?
Common IBS urgency triggers include dairy, caffeine, fried or high-fat meals, alcohol, and sugar alcohols like sorbitol and xylitol. Large or rich meals can set off urgency more than smaller, simpler ones, so portion size matters too. A food diary for IBS over 1 to 2 weeks can help you spot patterns, and a guided low-FODMAP diet trial can show whether FODMAPs are part of the problem. If urgency keeps happening, review your notes with a dietitian or healthcare professional.
3. Can Stress Make IBS Urgency Worse?
Stress, anxiety, and fear can make IBS urgency feel stronger, especially when you start watching every sensation and worrying about an accident. That can turn a strong urge into a hard-to-delay one, especially when you start watching every sensation and worrying about an accident. Deep breathing can calm your nervous system in the moment, and longer-term options like Cognitive-Behavioral Therapy, CBT for IBS, and gut-directed hypnotherapy can help reduce visceral hypersensitivity and break the stress-symptom cycle.
4. What Medications Help IBS Urgency?
An over-the-counter anti-diarrheal like loperamide can help when urgency is predictable before travel or a stressful event. If cramping or gut spasms are driving the urge, antispasmodics may help, and low-dose neuromodulators can calm gut nerve sensitivity over time. If bile acid malabsorption is possible, bile acid binders such as cholestyramine may be worth discussing, especially after gallbladder removal, and frequent or severe urgency should prompt a clinician visit for further IBS evaluation and tailored treatment.
