Gut motility in IBS-C, IBS-D, and IBS-M explains how bowel movement speed shapes constipation, diarrhea, and mixed symptoms. For many adults, the hard part is that bloating, urgency, or days without a bowel movement can happen even when scans look normal. Gut motility is the coordinated movement that pushes food, fluid, and waste through the digestive tract. The sections that follow show how the pattern changes, what may drive it, and what to do next.
The next sections compare slower transit in IBS-C with faster transit in IBS-D and the back-and-forth pattern in IBS-M. They also cover serotonin, methane, post-infectious change, stress, transit studies, manometry, breath testing, and capsule testing. Practical steps such as psyllium, hydration, Low-FODMAP changes, antispasmodics, and symptom tracking help turn the science into action.
For adults living with IBS, caregivers, and primary-care teams, the value is a clearer way to talk through stool patterns, triggers, and treatment choices. A working adult who alternates between straining and urgent diarrhea can bring a short symptom log and leave with a more focused plan for a gastroenterologist or registered dietitian. Clear next steps make the conversation easier and the follow-up more useful.
Gut Motility in IBS C D M Key Takeaways
- Gut motility controls how quickly food, fluid, and waste move through the digestive tract.
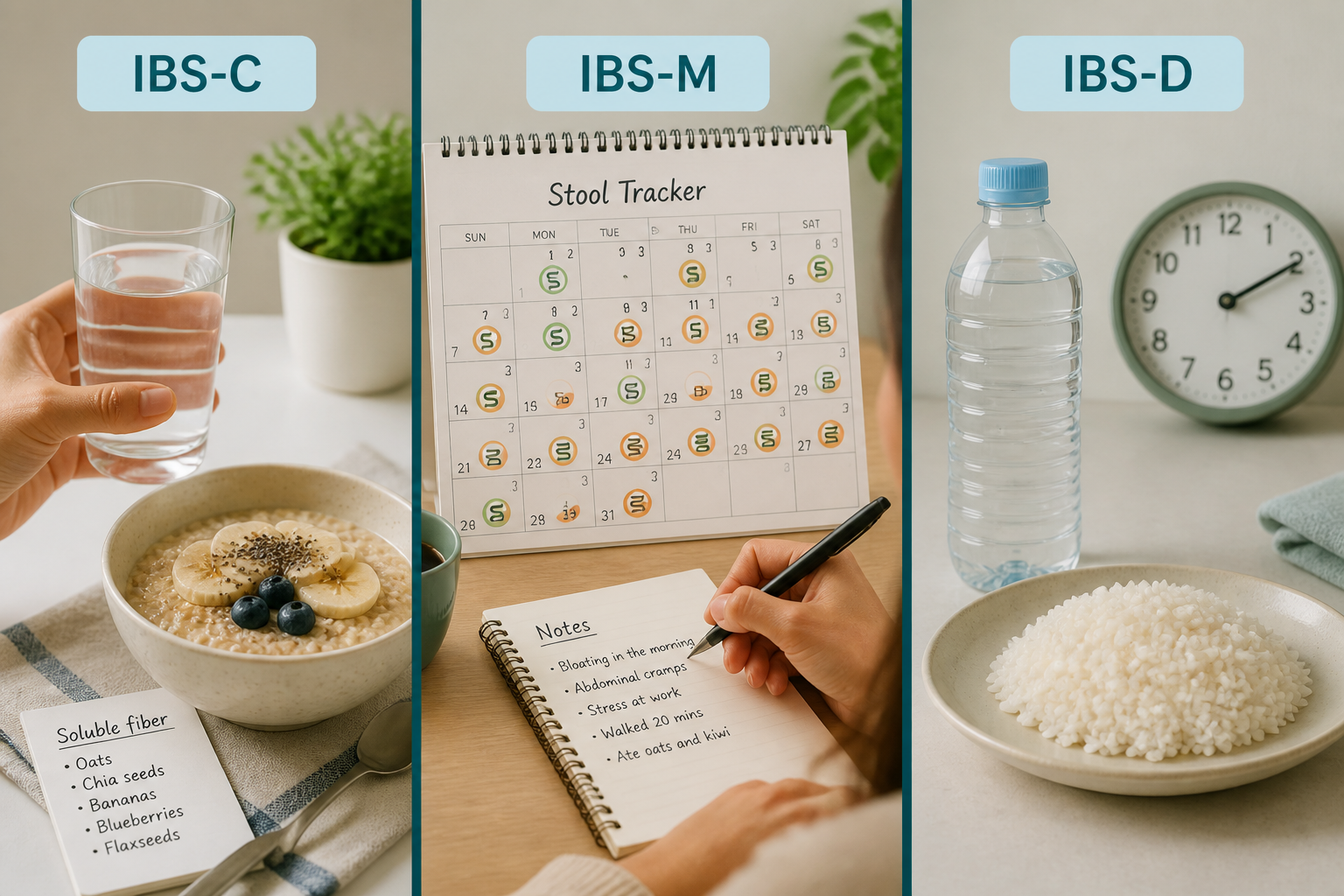
- IBS-C usually involves slower transit, harder stools, and more straining.
- IBS-D usually involves faster transit, urgency, and loose or watery stools.
- IBS-M shifts between constipation-like and diarrhea-like bowel patterns.
- Serotonin, microbes, methane, and stress can all alter motility.
- Transit studies, manometry, breath testing, and capsule tests can support evaluation.
- Blood in stool, severe pain, vomiting, or weight loss need prompt medical review.
What Is Gut Motility In IBS?
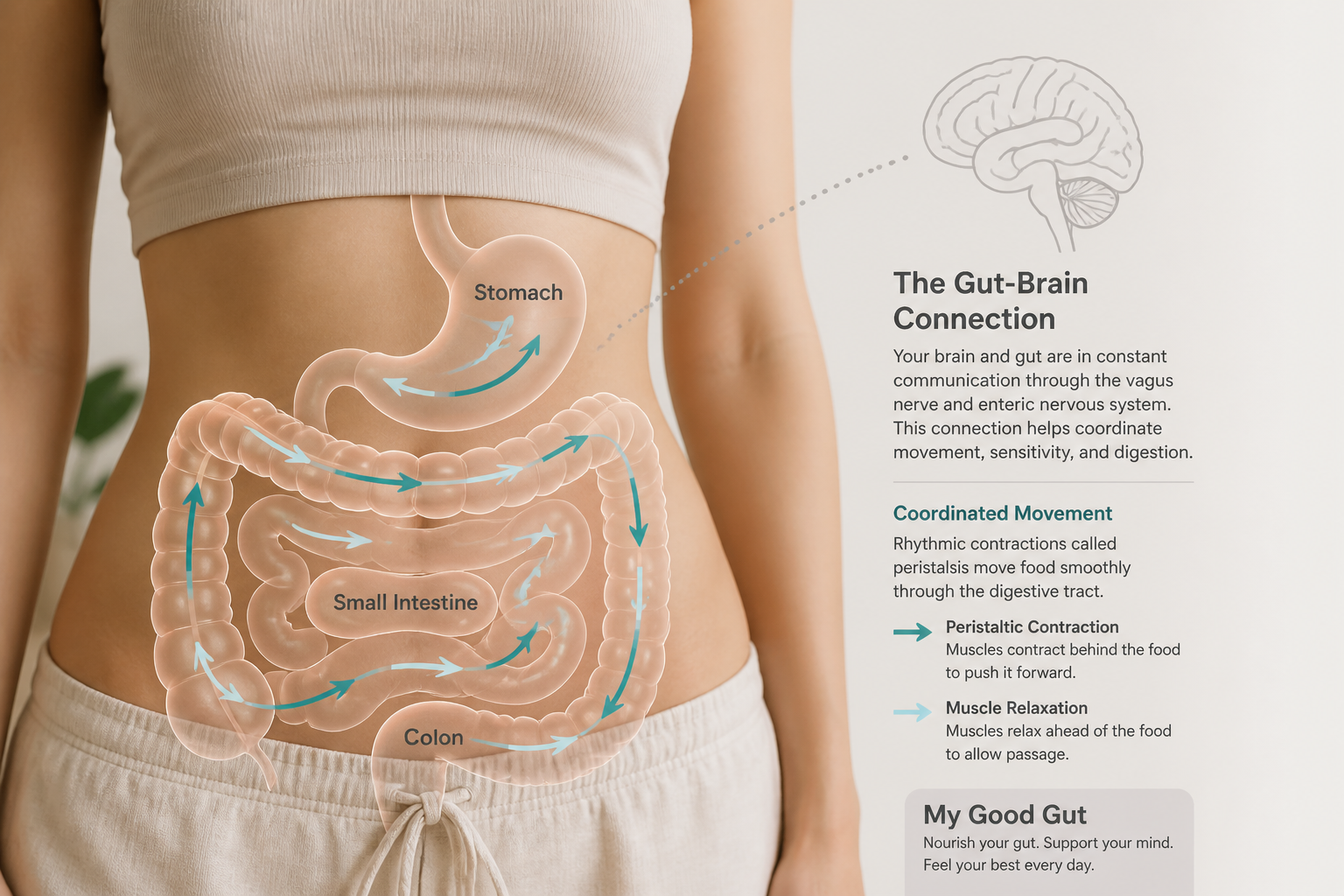
Gut motility is the coordinated, nerve-driven movement of muscle that mixes and pushes food, fluid, and waste through the stomach, small intestine, and colon until it becomes stool. When gut motility works well, you absorb nutrients and keep bowel movements on a steadier rhythm. In irritable bowel syndrome (IBS), that rhythm can change even when scans or biopsies look normal, which is one thread in how IBS develops.
IBS sits in the disorder of gut-brain interaction framework. That means signals between the central nervous system and the enteric nervous system can get disrupted. The enteric nervous system is the gut’s own nerve network, and it still responds to brain input through the vagus and spinal nerves. Stress, gut sensitivity, and bowel rhythm can all shape symptoms at the same time. Altered motility is only part of the picture. Visceral hypersensitivity, altered gut-brain interaction, microbial changes, and post-infectious factors also help explain why symptoms vary so much from person to person. Family patterns can matter too, and inherited IBS risk may help explain why IBS runs in some households.
Motility shifts often line up with the main IBS patterns:
- Faster transit can lead to loose stools and urgency.
- Slower transit can contribute to constipation and bloating.
- Mixed IBS can swing between both patterns.
That matters for diagnosis because motility helps clinicians make sense of abdominal pain, constipation, diarrhea, or mixed bowel habits as a functional bowel disorder rather than a structural disease. For many people, the motility pattern is the clue that points to the next step.
How Does Motility Differ In IBS-C, IBS-D, And IBS-M?
Motility is one of the main reasons IBS can look so different from person to person. It describes how fast stool moves through the gut. In IBS-C, IBS-D, and IBS-M, these patterns are tendencies, not fixed rules.
A quick comparison makes the pattern easier to see:
IBS subtype | What the bowel tends to do | What stool often looks like | Common clues |
|---|---|---|---|
IBS-C | Slower colonic transit | Hard, lumpy, or pebble-like stools | Straining, gas, cramping, bloating and constipation |
IBS-D | Faster colonic transit | Loose or watery stools | Urgency, frequent trips, sudden bathroom needs |
IBS-M | Swings between both patterns | Stool form changes over time | Constipation-like weeks and diarrhea-like days |
With IBS-C, slower colonic transit gives the colon more time to absorb water. That often leads to hard stools, straining, gas, cramping, and bloating and constipation. Pain may ease after a bowel movement.
IBS-D moves in the opposite direction. Faster transit can leave stool loose or watery, with urgency and a sudden need to get to the bathroom. IBS-M shifts between these patterns, so stool form and frequency can change from week to week or even day to day. Abdominal pain and bloating can happen in all three subtypes.
Most of the body’s serotonin, or 5-hydroxytryptamine, is found in the gut, and changes in serotonin levels or receptor sensitivity may help explain slower transit in IBS-C and faster transit in IBS-D (source). Changes in serotonin levels or receptor sensitivity may help explain slower transit in IBS-C and faster transit in IBS-D. Stress, diet, and other digestive factors can shift symptoms, so persistent, severe, or worsening changes should be evaluated by a qualified healthcare professional. Antispasmodics and a Low-FODMAP diet may help manage symptoms, depending on your pattern.
What Drives Altered Gut Motility In IBS?
Normal gut motility depends on coordinated muscle contractions in the intestinal wall. The enteric nervous system handles most of that rhythm, while the central nervous system adds input through the vagus and spinal nerves. When that coordination breaks down, movement through the gut can become too fast, too slow, or irregular.
A few major drivers help explain the pattern:
- Serotonin signaling: About 95% of the body’s serotonin, or 5-hydroxytryptamine, lives in the gut, and changes in release or receptor sensitivity can alter peristalsis. If serotonin release or receptor sensitivity changes, transit can slow in IBS-C or speed up in IBS-D.
- Microbes and metabolites: Shifts in the gut microbiome can change short-chain fatty acids and bile acids. Those changes can affect gut lining cells and nerves, which then alters muscle contractility, cramping, and how quickly contents move.
- Methane and other gases: Methane-producing archaea such as Methanobrevibacter smithii are strongly linked with slower transit because methane may reduce propulsion. Hydrogen-producing patterns can sometimes do the opposite and speed transit.
- Post-infectious change: Post-infectious IBS can start after gastroenteritis. Lingering inflammation and higher gut sensitivity can leave lasting changes in urgency, constipation, or mixed bowel habits.
- Stress and anxiety: Strong emotions can change the gut-brain interaction. That can increase contractions, delay gastric emptying, or make small bowel motility more erratic from flare to flare.
Taken together, IBS motility changes usually reflect several overlapping drivers rather than one single cause. Nerves, microbes, immune activity, and the brain-gut axis can all shift the pattern, which is why IBS causes can look different from person to person.
This content is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, so you should consult a qualified healthcare professional for persistent, severe, or worsening symptoms. Results vary by person, and any dietary or supplement advice should be individualized.
How Are Motility Tests Used to Diagnose IBS?
Motility testing can help show whether food or markers move too slowly or too quickly, but it rarely gives a clean IBS answer. IBS symptoms often come from several overlapping patterns, including altered gut movement, visceral hypersensitivity, gut-brain signaling changes, microbial shifts, and post-infectious effects after gastroenteritis. That is why diagnostic testing for motility disorders is most useful for finding a specific movement problem, not for proving IBS on its own.
Clinicians often use these tests:
- Transit studies: Sitzmarks and gastric emptying studies show whether material moves through the gut too slowly or too quickly. They can support suspected IBS-C or IBS-D, but a normal result does not rule out IBS.
- Manometry: This test measures muscle contractions in the esophagus, stomach, small bowel, or anorectum. It can show pressure or coordination problems, but findings in IBS can vary from day to day.
- Breath testing: This can help check carbohydrate malabsorption or possible SIBO. It does not diagnose IBS, and results can shift with diet, prep, and other conditions.
- Capsule testing: SmartPill tracks transit through the stomach, small bowel, and colon for a broader look at movement. It can show delayed or rapid transit, yet symptoms may still happen when results look normal.
A gastroenterology workup may combine several tests in a motility lab when symptoms are severe, atypical, or suggest another motility disorder. In practice, the question is often whether colonic transit, gastric emptying, or small bowel motility is off, or whether a post-infectious pattern needs a closer look.
How Can You Manage Motility Symptoms By Subtype?
The best plan does more than chase constipation or diarrhea. It aims to steady bowel transit, ease abdominal pain, and calm gut-brain triggers like stress and visceral sensitivity. Because IBS-C, IBS-D, and IBS-M can overlap, the best fit depends on your current pattern, triggers, and how well you tolerate treatment.
A simple subtype map works well:
Subtype | Main aim | Common tools |
|---|---|---|
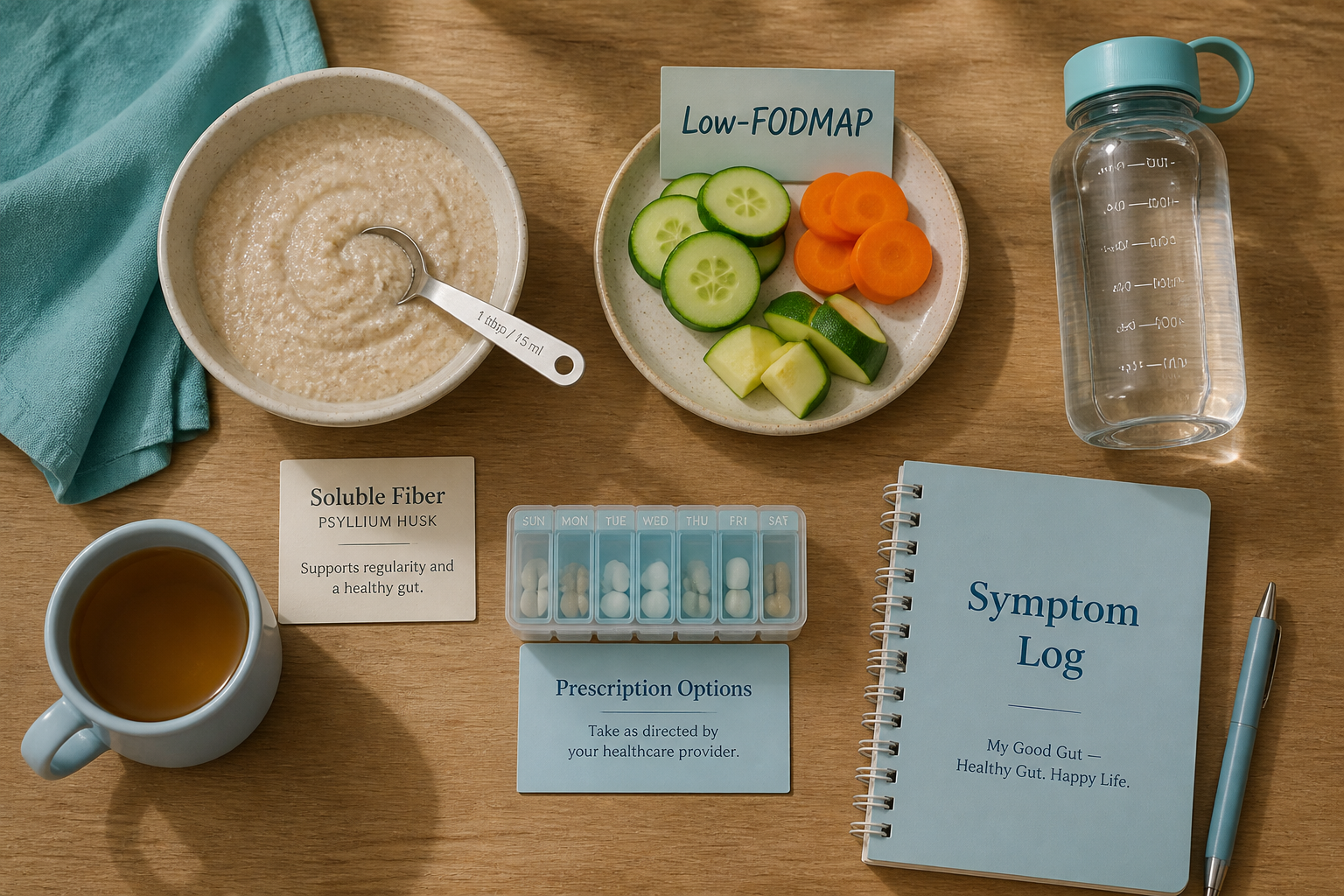
IBS-C | Soften stool and improve transit without adding more bloating | Soluble fiber such as psyllium, good hydration, osmotic laxatives, secretagogues like linaclotide or lubiprostone, and prokinetics such as prucalopride when appropriate |
IBS-D | Slow transit and reduce urgency | Less fatty food, less insoluble fiber, a Low-FODMAP diet, loperamide, antispasmodics, peppermint oil, and in selected cases alosetron |
IBS-M | Match treatment to the current phase | Soluble fiber or constipation-directed therapy during constipation flares, then anti-diarrheals, diet changes, or antispasmodics during diarrhea flares |
For IBS-C, the goal is better motility without making bloating or cramping worse. For IBS-D, the focus shifts to slowing transit and reducing urgency. IBS-M often needs a flexible plan that changes with the symptom pattern.
diet triggers for IBS can blur the picture, so your trigger list matters. When pain, bloating, and bowel changes seem tied to the brain-gut axis, behavioral care such as CBT or gut-directed hypnotherapy can help alongside medicine (source). CBT and gut-directed hypnotherapy are worth discussing when stress clearly worsens symptoms.
A practical decision path often looks like this:
- If constipation leads: Start with psyllium and fluids, then ask whether osmotic laxatives or prescription options fit your symptoms.
- If diarrhea leads: Limit fatty foods and insoluble fiber, then consider a Low-FODMAP diet, loperamide, or antispasmodics such as dicyclomine, hyoscyamine, or peppermint oil.
- If symptoms stay mixed or severe: Ask whether motility testing or breath testing makes sense to look for methane overgrowth, bile acid effects, or another cause.
A clinician-friendly checklist can keep the visit focused:
- Current pattern: IBS-C, IBS-D, or IBS-M, plus how often it changes
- Stool details: Frequency, urgency, and stool form
- Main triggers: Stress, meals, travel, menstrual cycle, or specific foods
- What you have tried: Fiber, diet changes, medicines, and supplements
- Next questions: Diet support, targeted drugs, CBT, gut-directed hypnotherapy, and whether more testing is warranted
My Good Gut is educational only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, and persistent, severe, or worsening symptoms should be reviewed by a qualified healthcare professional.
When Should You Seek Medical Help?
A short IBS flare can settle on its own, but a new or clearly worsening change in bowel habits should be reviewed by a clinician if it does not settle within days to 1 to 2 weeks, or sooner if other warning signs appear (source). Persistent constipation, diarrhea, or a new alternating pattern should not be ignored.
Get urgent care right away for:
- Blood in the stool or black stools
- Severe or steadily worsening abdominal pain
- Vomiting with a swollen abdomen
- Fever or signs of dehydration
Contact a clinician soon if you have unintentional weight loss, loss of appetite, nighttime symptoms that wake you up, or new fatigue that could point to anemia. IBS does not cause structural damage to the bowel, but new or worsening symptoms still need closer assessment so other causes are not missed (source).
Extreme constipation, several days without stool or gas, repeated blockage, severe bloating, or cramping can point to motility disorders such as gastroparesis, chronic intestinal pseudo-obstruction, or colonic inertia. Stress, anxiety, and other emotions can amplify symptoms through brain-gut signaling, but they do not explain every pattern. When symptoms are severe or atypical, diagnostic testing for motility disorders may include transit studies or manometry.
Gut Motility In IBS FAQs
These FAQs explain gut motility in IBS and the ways constipation, diarrhea, and mixed patterns can affect your symptoms. They also give you a simple starting point before the questions below.
1. Can IBS Cause Slow Gut Motility?
Yes, IBS can slow gut motility, especially in IBS-C, where fewer propulsive bowel movements move stool through the colon more slowly. When transit slows, the colon absorbs more water, which can leave stools hard, lumpy, and painful to pass, often with cramping or gas. Methane-producing archaea such as Methanobrevibacter smithii are linked to constipation and may slow intestinal muscle activity, and other microbial shifts, including hydrogen-producing bacteria or short-chain fatty acid patterns, can also change transit speed. IBS symptoms can be real even when imaging or biopsies look normal.
2. Can Slow Gut Motility Be Reversed?
Slow gut motility can often improve, but it is not always fully fixed. Progress usually comes from treating the likely driver over time and matching care to your symptoms, whether that means diet changes, laxatives or prokinetics for constipation, or other medicines for your motility pattern and pain level. About 95% of serotonin is made in the gut, so altered signaling can slow transit in IBS-C or speed it up in IBS-D. If methane SIBO is part of the picture, treatment may help bloating and sluggish transit, but results vary, and follow-up with a gastroenterologist or dietitian can help keep the plan individualized. This is for educational purposes only and is not a substitute for personalized medical advice.
3. What Does Type 7 IBS Poop Mean?
Type 7 on the Bristol stool scale means a fully watery stool with no solid pieces, which usually means stool is moving through your colon too quickly for normal water absorption. In IBS-D, nerve-driven contractions can speed transit, and that hypermotility can bring urgency along with cramping, bloating, and abdominal pain. Occasional loose stool can happen, but frequent Type 7 stools, dehydration, blood, fever, or worsening pain should prompt medical evaluation, and steady hydration, simple meals, and avoiding obvious trigger foods can help during a flare.
4. How Do You Tell IBS From Diverticulitis?
IBS usually causes recurring cramping, bloating, and pain that may ease after a bowel movement, while diverticulitis more often brings left lower abdominal pain, tenderness, fever, or a sick feeling. Warning signs that point away from IBS include worsening or fixed pain, vomiting, blood in the stool, or symptoms that become severe instead of coming and going. When diverticulitis is suspected, labs and an abdominal CT can help confirm inflammation, while IBS-related motility changes may not show up on testing. Transit studies or manometry are used selectively, and persistent or worsening symptoms need medical evaluation so infection or inflammation is not missed.
5. Does Bloating Signal Poor Gut Motility?
Bloating does not always mean slow gut motility. You can feel distended even when bowel movement speed is normal, especially if visceral hypersensitivity makes ordinary gas or contractions feel stronger. Dysbiosis can increase gas and change short-chain fatty acids and bile acids, and an exaggerated gastrocolonic response after meals can bring bloating, cramping, urgency, or a bowel movement. That is why bloating and constipation, diarrhea, alternating habits, and abdominal pain are best read as part of the broader IBS pattern, not as a stand-alone motility sign.
