Food sensitivity in IBS can make everyday meals feel unpredictable, especially when bloating, cramping, or urgency seem to show up without a clear pattern. Adults with IBS often end up cutting foods at random after one meal sets off symptoms. Food hypersensitivity is the umbrella term for allergy and intolerance, but IBS flares usually point to digestion or absorption problems rather than an immune attack. The sections ahead show how to separate likely triggers from red-flag symptoms and where to begin.
The next sections look at common triggers such as FODMAPs, lactose, fructose, polyols, and wheat fructans, then compare them with true allergy patterns. They also cover elimination and reintroduction, symptom logs, and when celiac or allergy testing fits the picture. A simple checklist helps keep the process focused and short-term instead of turning into another long food restriction.
For gastroenterologists, registered dietitians, and caregivers supporting busy adults with IBS, the value is a clearer way to sort meal-related symptoms from a true food allergy. One patient may react after milk and sugar-free gum, while another only flares after wheat-heavy meals, which points to different next steps. The path ahead gives a practical way to narrow triggers and have better conversations with a clinician.
Food Sensitivity in IBS Key Takeaways
- IBS food sensitivity usually reflects intolerance, not IgE-mediated allergy.
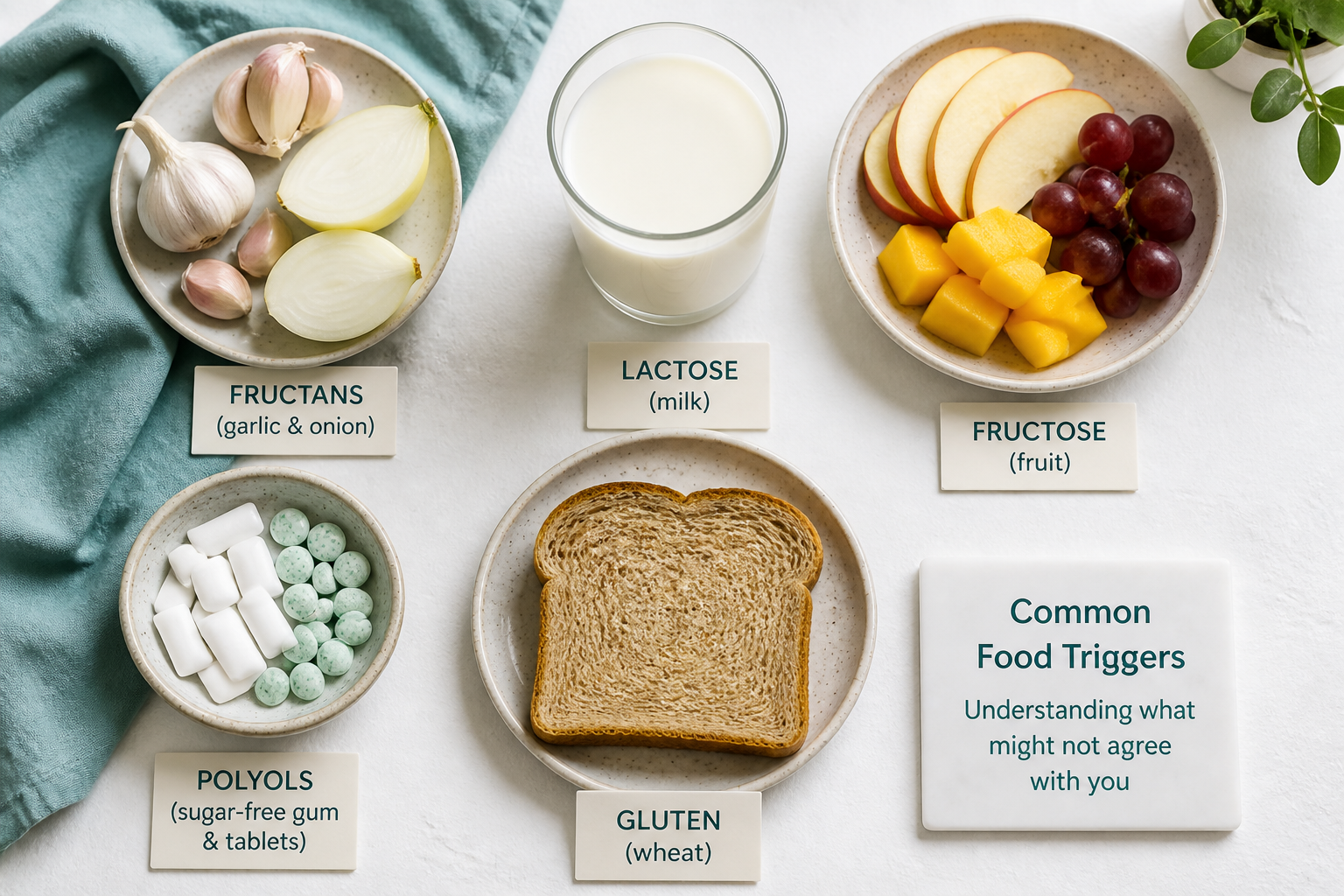
- FODMAPs are the first trigger group to suspect.
- Lactose, fructose, and polyols commonly cause bloating, gas, and diarrhea.
- Wheat symptoms often come from fructans, not gluten itself.
- Short baseline tracking makes elimination trials more reliable.
- Reintroduction one food at a time helps confirm real triggers and portions.
- Hives, swelling, wheezing, or vomiting call for allergy evaluation.
How Do You Tell Food Intolerance From Allergy?
Food allergy vs Food intolerance comes down to the mechanism and the timing. Food hypersensitivity is the umbrella term for both, but the causes are different. In an IGE-mediated allergy, oral tolerance has broken down and the immune system treats a food protein like a threat. In intolerance, digestion or absorption is the problem, not an immune attack.
For adults with IBS, true food allergy is uncommon, and intolerance is a more likely explanation for flares, which fits common drivers of IBS. A history of infection can also shape symptoms, and infection-triggered IBS is one reason symptoms can linger after a stomach bug.
The simplest way to separate the patterns is by what happens and when:
Pattern | More likely cause | Typical pattern |
|---|---|---|
Allergy | IgE-mediated allergy | Starts within minutes to 2 hours |
Intolerance | Digestion or absorption issue | Often shows up later and may depend on dose or meal size |
IBS flare | food sensitivity in IBS | Cramping, urgency, bloating, and bowel changes without skin or breathing symptoms |
IgE-mediated food allergy usually starts within minutes to 2 hours and can cause hives, swelling, breathing problems, vomiting, or low blood pressure (source, source).
Lactose and fructose are common examples because they can be poorly absorbed and harder for a sensitive gut to handle. Stress and fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) can make symptoms more noticeable. That pattern points more toward intolerance than allergy.
Red-flag symptoms need urgent medical care:
- Hives or itching
- Lip, tongue, or throat swelling
- Wheezing or trouble breathing
- Repeated vomiting, dizziness, or feeling faint
Those signs can reflect histamine release and mast cell activation, and they should not be dismissed as IBS. If symptoms are immediate, severe, or affect more than the gut, allergy evaluation makes sense. If they are delayed and mostly digestive, a food-and-symptom review is usually more helpful.
Persistent IBS symptoms still deserve a look for celiac disease and IBS overlap. Celiac disease affects about 1% of the general population, and it is reported more often in people with IBS than in the general population, so celiac testing is often considered when symptoms fit (source, source).
This content is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, so you should see a qualified healthcare professional for persistent, severe, or worsening symptoms. Results vary by person, and any dietary advice should be individualized.
Which IBS Trigger Foods Should You Suspect First?
The first foods to suspect are usually Fermentable carbohydrates in your IBS food triggers. These poorly absorbed carbs can pull water into the bowel and ferment quickly. That often leads to bloating, cramping, gas, and loose stools after meals.
A practical ranking looks like this:
Priority | What to suspect | Why it matters | Common symptom pattern |
|---|---|---|---|
1 | FODMAPs | A Low-FODMAP diet focuses on the most common trigger group in IBS, and these carbs can set off symptoms fast when they are poorly absorbed | Bloating, pain, gas, loose stools |
2 | Lactose | Lactose intolerance often shows up after milk, ice cream, soft cheese, or creamy foods, especially in larger servings | Bloating, gas, abdominal pain, diarrhea |
3 | Excess fructose | Fructose intolerance is more likely when apples, mango, honey, fruit juice, or sweetened drinks push intake past what you can absorb | Bloating, gas, diarrhea |
4 | Polyols | Sorbitol and mannitol often hide in sugar-free gum, mints, stone fruits, mushrooms, and cauliflower | Gas, bloating, diarrhea |
5 | Gluten-containing grains | Wheat-heavy meals can still be a problem, but the issue is often wheat fructans rather than gluten itself | Bloating, pain after meals |
Lactose is worth a close look if dairy keeps setting off the same pattern. Constipation is less typical than bloating, gas, and diarrhea. That is why lactose intolerance often stands out when milk or creamy foods are the repeat offender.
Fructose and polyols tend to behave like an osmotic load. They draw extra water into the bowel and can leave you feeling distended or urgent. That pattern is common with fruit juice, sugar-free products, and some fruits and vegetables.
Gluten-containing grains are a secondary suspect unless bread, pasta, or wheat-heavy meals reliably cause trouble. For many people, the real issue is wheat fructans, not gluten itself. That is why non-celiac gluten sensitivity can look a lot like a FODMAP reaction, with bloating and pain after meals instead of a classic allergy pattern.
The symptom mix matters because different triggers act differently in the gut. Fermented FODMAPs and excess fructose usually drive bloating, gas, and pain. Lactose and polyols more often add diarrhea.
IBS reactions are usually tied to non-immunoglobulin E sensitivity, visceral hypersensitivity, and gut-brain signaling changes rather than a true food allergy. That is also why IBS and diet works best as a careful process, not a guess. A structured Low-FODMAP diet can help you narrow the field, but the goal is to find your pattern without cutting out more than you need.
How Do You Run A Safe Elimination Trial?

A safe elimination trial works best when it stays short, structured, and easy to measure. An elimination diet should act like a temporary test, not a permanent rule. That approach gives you cleaner clues for the diagnosis of food intolerance and makes the results easier to trust.
A simple sequence helps keep the trial focused:
- Build a baseline first. Track your usual meals, bowel habits, symptoms, and timing for at least 1 to 2 weeks before changing your diet so you can compare baseline symptoms with the elimination phase (source, source).
- Keep the exclusion phase time-limited. A short, time-limited elimination phase is commonly used, and public patient guidance often places the trial in a range of about 2 to 6 weeks depending on the diet and the suspected trigger (source, source).
- Remove the most likely triggers first. High-FODMAP foods are often the first place to start. Lactose is another common target if dairy seems suspicious. A single, focused approach gives you a clearer read on what is helping.
- Use testing when it fits the story. If fructose intolerance seems possible, a breath test may help your clinician sort out what is going on. That kind of result can support clinical dietary management, but it still needs to be interpreted alongside your history and other test results when needed.
Some situations call for extra caution before you begin. A qualified healthcare professional or registered dietitian should review your plan first if you have a history of eating disorders, unintended weight loss, pregnancy, diabetes, celiac disease concerns, or an already restricted diet. Those situations can raise the risk of nutritional gaps or a missed diagnosis.
Stop the trial and seek medical care if you notice these safety flags:
Safety flag | Why it matters |
|---|---|
Blood in the stool | May signal bleeding or inflammation |
Fever | Can point to infection or another illness |
Persistent vomiting | Raises dehydration risk |
Severe pain | Needs prompt evaluation |
Dehydration | Can become serious quickly |
Nighttime symptoms that wake you | Can suggest something beyond IBS |
Symptoms getting worse | Means the plan is not staying safe |
Treat the trial as a diagnostic step, not a long-term restriction. If symptoms stay unclear or severe, your clinician may review a detailed food history, rule out celiac disease and allergy, or use supervised food challenge testing to guide the next step.
How Do You Reintroduce Foods And Track Reactions?
A careful reintroduction plan helps you find real triggers without getting stuck in an overly strict Elimination diet. In IBS, symptoms can come from food intolerance, Visceral hypersensitivity, portion size, stress, or poor sleep. The goal is to test one variable at a time and keep the rest steady.
A practical challenge plan looks like this:
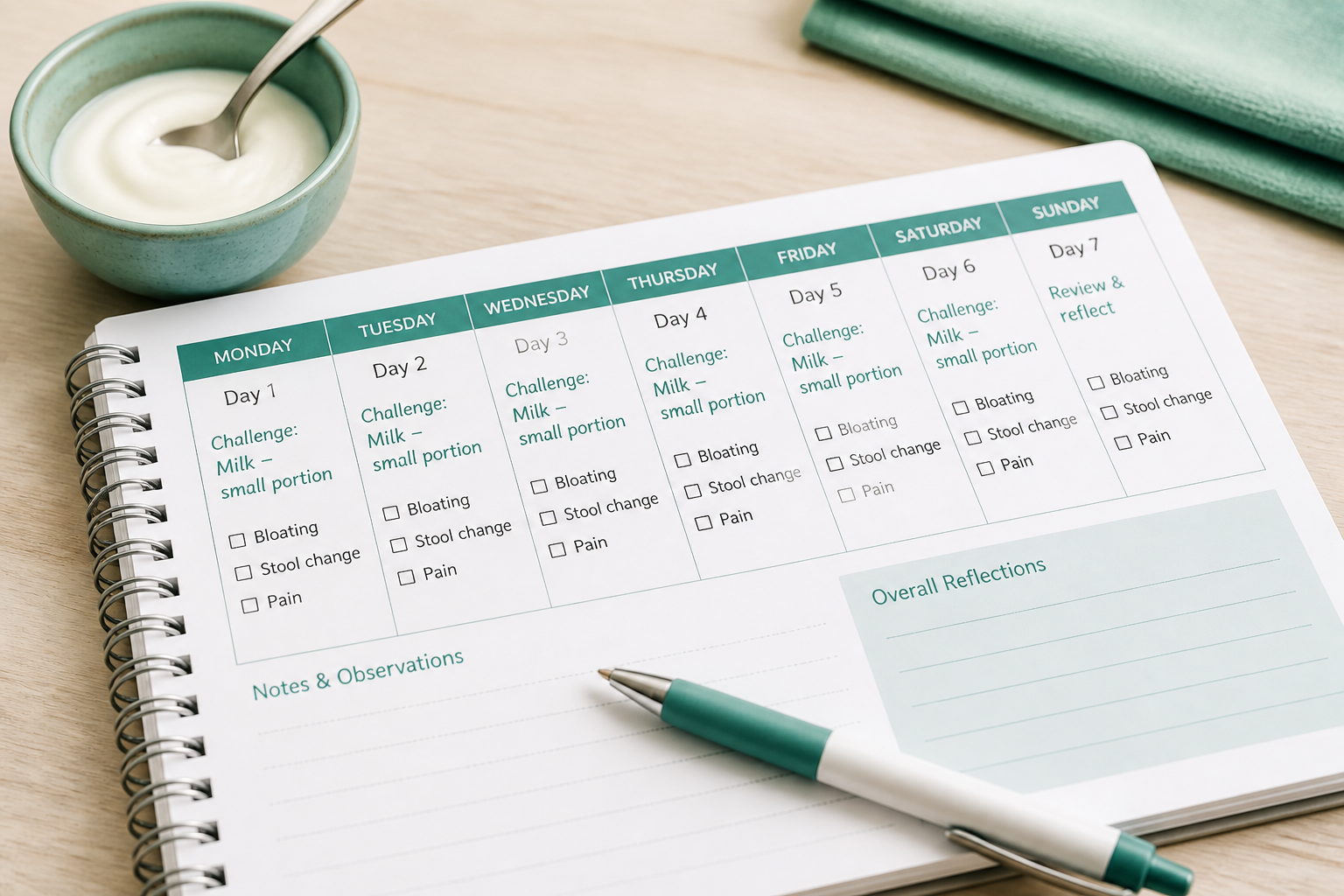
- Pick one food or one FODMAP group and keep the rest of your meals unchanged.
- Start with a small portion. If symptoms stay mild or absent, move to a normal serving later that day or on the next challenge day.
- Spread each test across several days so you can catch reactions that show up hours later or the next day.
- Repeat only when needed. A clear, repeatable flare matters more than one strange day.
A simple symptom log makes patterns easier to spot than guesswork. Track the food, portion size, time eaten, bowel changes, bloating, pain, urgency, nausea, stress, sleep, travel, and other changes that could muddy the picture.
What you notice | What it may mean |
|---|---|
Strong symptoms after the same food more than once | Likely trigger |
Mild symptoms once, then no issue later | Possible portion issue or normal IBS variation |
Symptoms the next day | Delayed reaction, so keep watching beyond mealtime |
Mixed or vague symptoms | Could be stress, sleep loss, or background IBS variation |
That pattern matters because not every reaction means true intolerance. A strong, repeatable flare after the same food points toward a likely trigger. A one-off reaction may reflect normal IBS variation or a larger serving. If you notice hives, swelling, wheezing, or vomiting, stop the challenge and seek medical care because those signs fit allergy better than IBS.
Dietitian-led reintroduction protocols are often a smart next step. They can confirm your tolerance levels, reduce unnecessary food restriction, and help you build a more personalized long-term plan. That support is especially useful if you are considering IGG food antibodies or IGG4 testing, because their value in IBS is still controversial.
Stop the challenge if symptoms become severe, persistent, or disruptive. Reach out to a gastroenterologist or registered dietitian if you have multiple suspected triggers, cannot isolate the culprit, or need help deciding whether your symptoms fit IBS intolerance or another problem.
Which Tests Help, And Which Ones Mislead?
The best tests in IBS match a clear symptom pattern. Tests that only show sensitization can muddy the picture and lead to food avoidance that is bigger than the problem.
Test | When it helps | Where it misleads |
|---|---|---|
Skin-prick testing or specific IGE blood testing | Suspected IGE-mediated allergy with fast symptoms like hives, swelling, wheeze, or vomiting | Bloating, pain, or bowel changes without allergy-type reactions |
Celiac serology | Symptoms that overlap with IBS or chronic diarrhea | A negative result does not explain every trigger |
Lactose breath test | Dairy-linked gas, bloating, or diarrhea | It does not prove a milk allergy or explain all IBS symptoms |
IGG food antibodies and IGG4 panels | Rarely useful in routine IBS care | They often reflect exposure, not a real trigger |
Supervised food challenge | Clear food-linked symptoms that need confirmation | Broad, unsupervised food exclusion |
Celiac disease and IBS can look alike, so celiac serology can help when the story fits. People with IBS may be about four times more likely to have celiac disease than the general population. A positive result needs proper follow-up, not guesswork.
For updated review articles on test limits and symptom overlap, the NCBI RSS feed can be a useful source.
A lactose breath test can help when milk or ice cream seems to trigger gas, bloating, or loose stools. It points to lactose malabsorption, not IGE-mediated allergy, and not the full diagnosis of food intolerance by itself. Some people react to the test dose but still handle small amounts of dairy in daily life.
The weakest panels are the ones built around IGG food antibodies and IGG4. Those antibodies can show up in healthy people, and higher levels have been linked to atopy without proving a food is causing your symptoms. In practice, a positive panel usually reflects exposure, not a reason to cut out half your diet.
False results matter here. A positive allergy test does not always mean the food is driving IBS, and a negative test does not rule out intolerance, FODMAP sensitivity, or delayed reactions. In some niche cases, clinicians may discuss Colonoscopic allergen provocation (COLAP), but that is not a routine IBS test. HHS also stresses that persistent, severe, or worsening digestive symptoms deserve medical review (HHS).
The safest approach is still straightforward:
- Start with a careful food and symptom history.
- Test only when a specific concern points to a real diagnosis.
- Use a structured elimination and reintroduction plan when food triggers are unclear.
- Follow up with a qualified healthcare professional if symptoms are severe, persistent, or worsening.
That approach protects you from unnecessary restriction and gives you a clearer path to the right answer.
How Do You Build A Long-Term Eating Plan?
A long-term IBS plan works best when restriction gets smaller over time, not bigger. After the elimination phase, keep the foods that stayed calm, avoid only the specific triggers you confirmed, and let the rest of your diet return to normal as much as possible. That keeps IBS and diet goals on track without creating avoidable nutrition gaps.
The steady version of the plan usually starts with a short list of tolerated staples. Add one new food at a time, then wait long enough for symptoms to settle so you can judge the result clearly. That pattern helps with IBS food triggers, and it fits Clinical dietary management because the goal is control without needless restriction.
Common trigger-food buckets often matter more than one food on its own. Those buckets can include Fermentable carbohydrates, lactose, fructose, gluten-containing grains, and portion size, so reintroduction can stay focused. The Low-FODMAP diet is one useful way to sort those patterns, especially when symptoms shift from meal to meal.
A simple reintroduction pattern looks like this:
Reintroduction result | What it usually means |
|---|---|
No symptoms | The food can usually stay in your personal rotation |
Mild or delayed symptoms | A smaller portion may work better |
Clear repeat reactions | The food is more likely a true long-term trigger |
Nutrition still matters, especially if several foods stay off your list. Replace removed foods with close alternatives and keep an eye on fiber, protein, calcium, iron, and meal variety. That matters even more with Post-infectious IBS or Gut barrier dysfunction, because it is easy to cut back too far when symptoms flare. Patient-friendly education can also help you make sense of the bigger picture, including trusted resources like NLM on YouTube.
The downloadable elimination and rechallenge workbook makes the pattern easier to spot. Track these details for each test food:
- Symptom severity: mild, moderate, or strong
- Bloating, stool frequency, and stool form: the most useful day-to-day IBS markers
- Meal timing: what else happened before and after you ate
- Test food and portion size: whether the reaction seems dose-related
- Symptom timing after eating: how soon the change showed up
Bring in a registered dietitian or healthcare professional if your diet is getting very limited, your weight is dropping, deficiencies are a concern, symptoms could reflect food sensitivity instead of allergy or celiac disease, or several reintroductions still feel unclear. Their guidance helps you protect nutritional adequacy while you sort your long-term plan.
Food Sensitivity in IBS FAQs
These FAQs cover the most common questions about food sensitivity in IBS and Food hypersensitivity. They also look at genetic risk for IBS, which can help explain why triggers and symptoms vary from person to person.
1. Can food sensitivities trigger IBS symptoms?
Yes. Food sensitivities can trigger or worsen IBS symptoms, and studies suggest that up to 65% of people with IBS notice food-related flares, even though IBS affects about 10% to 20% of U.S. adults. The issue is usually not a true IGE-mediated food allergy, but poorly absorbed carbohydrates like FODMAPs and lactose often drive the flares. Because your response is personal, one food may bother you on some days and not others, so the goal is to spot your own patterns without blaming every digestive symptom on food alone.
2. Why do IBS symptoms appear hours later?
You can notice IBS symptoms hours after eating because food has to move through the small intestine and reach the colon, where gut bacteria ferment certain carbohydrates. Visceral hypersensitivity can make normal stretching feel painful, and IBS pain perception helps explain why a little gas can feel like a lot. IBS and gut movement can also change how fast food moves, while Gut microbiota, Gut barrier dysfunction, Post-infectious IBS, and Mast cell activation may heighten symptoms, and a delayed immune response is not the same as an IGE food allergy or the main cause for most IBS reactions.
3. Does IBS cause diarrhea or constipation?
IBS can show up as diarrhea-predominant IBS (IBS-D), constipation-predominant IBS (IBS-C), or a mixed pattern, so the same diagnosis can look very different from person to person. Poorly absorbed carbohydrates such as fructose, lactose, sorbitol, and other FODMAPs often worsen symptoms, but the pattern matters: IBS-D is more likely to flare with caffeine, very fatty meals, and high-FODMAP foods that trigger urgency, loose stools, and cramping. With IBS-C, low-fiber eating, heavy dairy intake, and larger amounts of fermentable foods may add gas and bloating while constipation sticks around, and mixed IBS can shift over time as your trigger foods change.
4. Can stress worsen food reactions in IBS?
Stress can make food reactions feel stronger in IBS because gut-brain signaling can raise visceral sensitivity, so the same meal may feel rougher on a high-pressure day. That does not mean the food is always the main problem, and cramping, bloating, or urgency can flare after eating when stress is high; the stress-related IBS triggers explains that connection in more detail. Eating slowly, keeping meals regular, and taking a few minutes for deep breathing or a short walk before meals can help, and if flares keep clustering on busy days, track stress alongside foods and speak with a qualified healthcare professional if symptoms persist or worsen.
5. Should you try a low-FODMAP diet first?
A low-FODMAP diet is often a sensible first step if your IBS symptoms flare after meals, especially with bloating, pain, gas, or loose stools. Lowering FODMAPs can help when several common food triggers may be involved. It is not a cure, so the best approach is a short elimination phase followed by planned reintroduction, ideally with guidance from a clinician or dietitian, and you should get medical evaluation first if you have weight loss, blood in stool, anemia, or worsening symptoms.
Sources:
- NCBI on GitHub: https://github.com/ncbi
- NCBI RSS feed: https://ncbiinsights.ncbi.nlm.nih.gov/
- NCBI on X (formerly known as Twitter): https://twitter.com/ncbi
- NLM on Facebook: https://facebook.com/nationallibraryofmedicine
- NCBI on Facebook: https://facebook.com/ncbi.nlm
- HHS: https://hhs.gov/
- HHS Vulnerability Disclosure: https://hhs.gov/vulnerability-disclosure-policy/index.html
- NCBI on LinkedIn: https://linkedin.com/company/ncbinlm
- USA.gov: https://usa.gov/
- NLM on YouTube: https://youtube.com/user/NLMNIH
