IBS genetics, hereditary risk, and family history are the focus of this plain-language guide. Many people with IBS want to know whether a parent’s symptoms, a sibling’s diagnosis, or a long family pattern means the condition is inherited. Heritability means how much genes shape risk across a group, not whether one person is destined to get IBS, and the evidence here helps separate real risk from guesswork.
The sections ahead cover twin and family studies, GWAS findings, candidate genes such as SCN5A and SLC6A4, and the brain-gut pathways that may shape symptom risk. It also shows why results vary across studies and why no single IBS gene explains most cases. Expect a practical read on what family history can signal, what warning signs matter, and which details are worth bringing to a healthcare professional.
For adults living with IBS, family members trying to make sense of the pattern, and clinicians who need a clear summary, the key value is separating inherited risk from false certainty. A parent with IBS and a child with new bloating can use the family-history questions in this topic to decide whether tracking symptoms or scheduling a review comes first. That keeps the conversation grounded in symptoms, triggers, and sensible next steps.
IBS Genetics and Family History Key Takeaways
- IBS risk is polygenic, with many small variants adding modest risk.
- Heritability measures group risk, not a personal prediction.
- Family clustering often reflects shared genes, habits, and exposures.
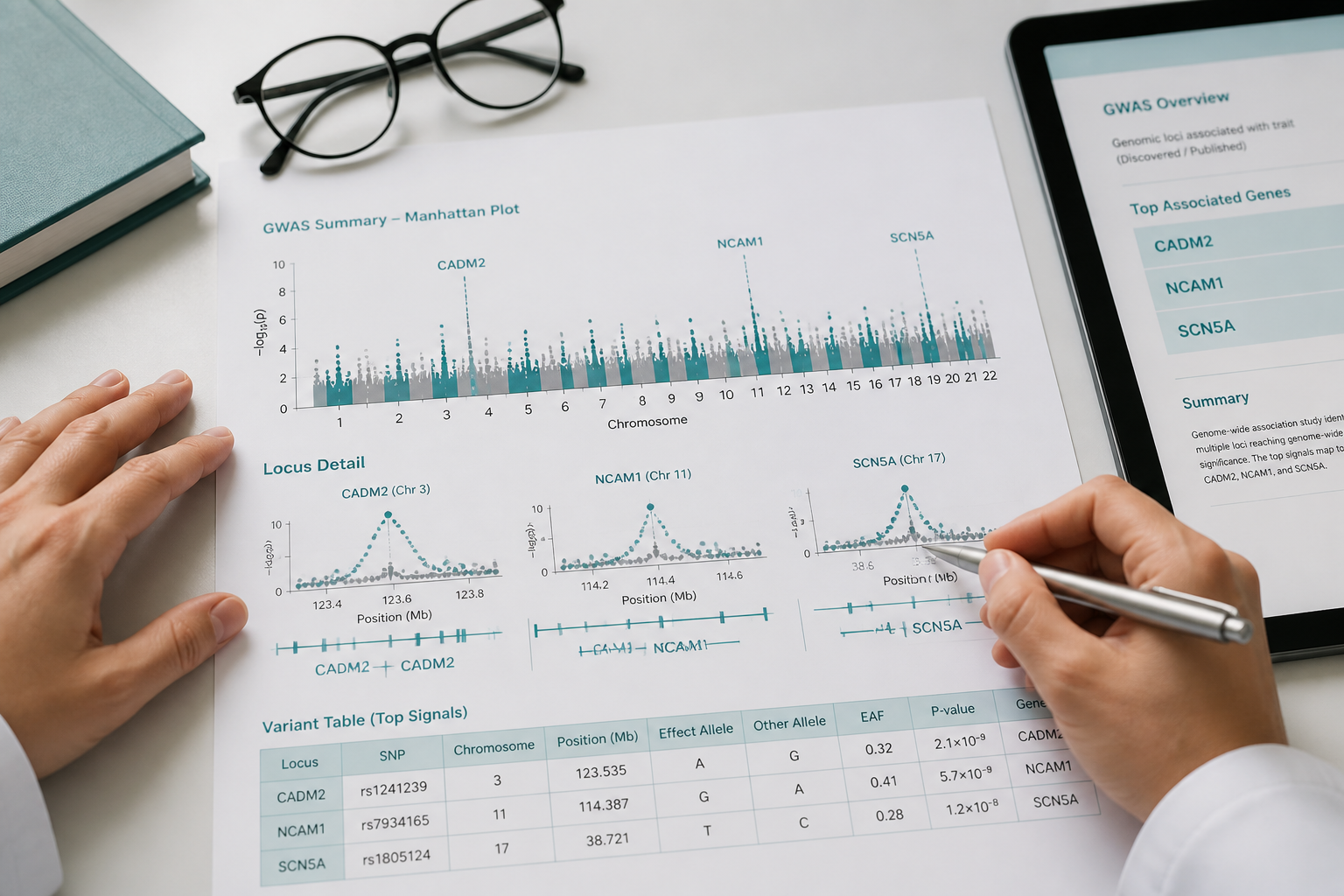
- GWAS points to brain-gut pathways and loci like CADM2 and NCAM1.
- Candidate genes such as SLC6A4 and SCN5A have mixed evidence.
- No routine genetic test can diagnose IBS for most people.
- First-degree family history should trigger symptom tracking and clinician review.
Is IBS Genetic Or Hereditary?

Irritable bowel syndrome (IBS) appears to have a genetic component, but it does not follow a single-gene, Mendelian pattern. In IBS genetics, many small genetic effects work with a gene-environment interaction, so stress, diet, infections, and other exposures help shape whether symptoms show up. That is why the origins of IBS matter so much alongside family history.
Heritability means how much of the difference in risk across a group may be linked to genes, not how “destined” one person is to get IBS. The research on irritable bowel syndrome heritability is mixed, which is why the numbers vary so widely. A PubMed-indexed review also shows how uneven the early twin and family data are, which helps explain the spread in estimates (PubMed).
Twin and family studies suggest that IBS has a genetic component, but published estimates vary widely across study designs and populations (source).
Those numbers do not mean IBS is either “genetic” or “not genetic.” They show that the condition sits in a middle zone, where genes matter but do not explain everything.
Family clustering can look like inheritance, but it is not the same thing:
- Shared genes: Relatives may carry similar risk variants.
- Shared routines: Meal patterns, sleep habits, and activity levels often overlap.
- Shared exposures: Infection history, stress, and early-life events can run through a household.
That is why IBS can run in families without a parent passing down an IBS gene in a simple way. The condition may cluster, but it is not inevitable.
IBS is best described as a polygenic condition, which means many common variants each add a tiny bit of risk. In plain language, polygenic risk changes probability, not destiny. A large genome-wide association study meta-analysis included 53,400 IBS cases and 433,201 controls. Replication in 23andMe data covered 205,252 cases and 1,384,055 controls.
Similar small-effect patterns have also been reported in UK Biobank analyses. Even with that scale, the strongest signals still point to modest-effect risk loci rather than a diagnostic gene.
For you, the practical takeaway is simple. A family history of IBS should raise awareness and make risk conversations more careful, but it does not prove strict heredity. It is one clue among many, and it should sit next to symptoms, stress load, diet patterns, and medical history when you think about next steps. This overview is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, so persistent, severe, or worsening symptoms deserve a qualified healthcare professional’s review.
How Much Does Family History Matter?
Family history matters, and the pattern in relatives can help guide what to watch for. The irritable bowel syndrome heritability signal looks modest, and diet, stress, household routines, and other environmental factors still shape whether symptoms appear and how strong they feel. Diet, stress, household routines, and other environmental factors still shape whether symptoms appear and how strong they feel.
A simple way to read the family pattern is this:
- Family history appears to matter in IBS.
A PubMed-indexed family study reported the same pattern, with about 50% of people with IBS naming an affected relative and first-degree relatives showing a higher rate than control relatives (source).
For you, that means family history should raise awareness, not create certainty. Having a parent, sibling, or child with IBS raises your odds, but it does not make IBS inevitable. Most relatives of people with IBS never develop the condition.
Share these details with a healthcare professional if your symptoms are lingering or changing:
- Which relative has symptoms, especially whether it is a first-degree relative
- When the symptoms started in that family member
- Whether the pattern is mostly diarrhea, constipation, bloating, pain, or mixed bowel changes
- Whether there are warning signs like blood in the stool, weight loss, fever, or waking at night with symptoms
If IBS-like symptoms run in your family and your own symptoms feel persistent, worsening, or unusual, earlier medical evaluation is the safer path. That conversation can help rule out other causes of abdominal pain and bowel changes before anyone assumes it is just IBS.
Which Genes And Studies Matter Most?
The strongest IBS gene associations come from GWAS, not from small single-gene studies. These genome-wide scans test many variants at once, so they are less likely to be fooled by false positives than older candidate-gene reports. For you, the main message is simple: IBS genetics looks real, but it points to shared brain-gut signaling rather than one IBS-only gene.
A simple way to scan the evidence is this:
Finding | What it suggests | Confidence |
|---|---|---|
CADM2 and NCAM1 | Brain and nerve signaling may shape symptom risk | Stronger, because these signals have shown up in large studies |
PHF2/FAM120A, DOCK9, CKAP2/TPTE2P3, BAG6 | Risk is spread across several pathways, not one high-impact mutation | Moderate to strong, because they fit the same polygenic pattern |
SCN5A | Sodium-channel changes may affect bowel movement patterns in a subset of people, especially some with IBS-D | Interesting, but less reproducible and not yet broad enough for routine use |
SLC6A4 and other candidate genes | Serotonin signaling and stress response may matter, but results are mixed | Lower confidence, because findings often shift from study to study |
The broad pattern behind IBS gene associations is polygenic. That pattern helps explain why no single mutation drives most cases. It also helps explain why IBS can look different from one person to the next.
The strongest population studies usually come from 23andMe and UK Biobank, because those data sets include enough cases to detect small signals. One large study reported six associated regions, including NCAM1, CADM2, PHF2/FAM120A, DOCK9, CKAP2/TPTE2P3, and BAG6. Researchers also use colocalization GTEx analysis to ask whether a DNA signal lines up with gene activity in a relevant tissue. That kind of follow-up can help move a result from “interesting marker” to “possible mechanism,” but it still does not prove one gene causes IBS on its own.
SCN5A is a good example of why the details matter. A few reports link SCN5A mutations with IBS, including IBS-D, and they suggest that sodium-channel changes may affect intestinal motility in IBS in a subset of people. The signal is worth watching, but it is not as widely repeated as the GWAS hits. That makes it a subset finding, not a general IBS marker.
Candidate-gene studies such as SLC6A4 helped shape early ideas about serotonin, stress, and bowel activity. Their weakness is consistency. Across studies, the results have often been mixed, so they work better as clues than as solid proof. The practical takeaway is reassuring. Your family history may matter, but IBS genetics does not yet support a diagnostic genetic test or a reliable prediction of your personal IBS risk.
What Do GWAS And Candidate Genes Show?
GWAS of IBS has pushed the field far beyond older candidate-gene work, but the signal is still modest. One discovery cohort included about 53,400 people, which is large by gut genetics standards. Even so, the results point to small effects rather than a single clear cause. That pattern fits polygenic risk, where many variants each add a little to overall susceptibility.
The heritability numbers set the right expectations. SNP heritability was estimated at about 5.77% in the discovery cohort, and cohort-specific estimates ranged from roughly 3.14% to 7.71%. In plain terms, common variants explain part of your risk, but not all of it. Family history matters, but it is only one piece of the IBS picture.
Candidate-gene studies have focused on pathways that make biologic sense for IBS. These include serotonin signaling, stress response, and the brain-gut axis. Genes such as SLC6A4, SCN5A, HTR3B, COMT, ADRA2A/C, NPSR1, and KLB have all shown up in IBS gene associations. A classic PubMed-indexed review of early work pointed to serotonin-related pathways, while also showing how uneven the evidence can be (PubMed).
Replication remains the main limit. Many individual SNP effects are tiny, so one study can find a signal that another study misses. Results can also shift with ancestry, sample size, and study design. Direction can even differ across papers, which is why no single IBS gene has been confirmed.
That is where endophenotype work helps bridge the gap between genes and symptoms. Endophenotypes are smaller, measurable traits that sit closer to biology than the IBS label itself. GI transit and brain imaging can help show how a variant might affect motility, pain processing, or brain-gut signaling. That is also why heightened gut sensitivity matters, since it links symptoms to a clearer biological process.
IBS subtypes genetics may matter too, because constipation-predominant and diarrhea-predominant patterns may not share the same risk signals.
A simple way to read the evidence is this:
- GWAS: Best for finding broad risk signals across large groups
- Candidate genes: Best for generating biologic ideas about serotonin, stress, and motility
- Transit and imaging studies: Best for connecting variants to function in the gut and brain
Taken together, these study types support a real genetic component without overstating it. They also explain why IBS often reflects a mix of inherited risk, brain-gut signaling, and environmental triggers rather than one fixed cause.
What Does IBS Genetics Mean For You?
Genetics can shift your odds, but it cannot give you a yes-or-no answer for IBS. Most IBS risk is polygenic, so the practical focus stays on symptoms, triggers, and treatment response. Those differences also interact with diet, stress, gut infection, and other triggers.
A family history matters, and regular tracking can help you spot symptoms early for you or your children. Relatives often share genes and daily habits, so an IBS diagnosis in the family should raise awareness and encourage earlier symptom tracking. It should not make IBS feel inevitable.
What genetics can tell you | What genetics cannot tell you |
|---|---|
Your risk may be a little higher or lower than average | Whether you will definitely develop IBS |
A family pattern may point to shared risk | A guaranteed prediction for children or siblings |
A rare variant may help explain unusual cases | A routine screening answer for most people |
Some gene results may help guide a medicine choice | The best treatment for every person |
That is why IBS genetics is most useful for context. It can help explain why symptoms show up in some families, but it should never replace the basics of care, such as your symptom pattern, trigger foods, stress load, bowel habit changes, and response to treatment.
SCN5A has been reported in a small IBS subgroup, but the finding is research based and does not support routine genetic testing for most people with IBS (source).
That matters because rare findings can sound bigger than they are. For most people, SCN5A testing will not change day-to-day care. It is usually not part of routine IBS workups unless symptoms, family patterns, or unusual test results point in that direction.
Genetics can be more helpful when it may affect treatment choice. This is where pharmacogenomics IBS comes in, which means using gene information to see how your body may process a medicine.
A few situations stand out:
- CYP2D6: This test may matter if a clinician is considering tricyclic antidepressants for visceral pain. Poor metabolizers can clear these drugs more slowly, which may raise the risk of side effects or toxicity.
- SLC6A4: This serotonin transporter gene has been studied as one of the genetic predictors of treatment response for alosetron and tegaserod. The signal is real enough to study, but the evidence is mixed and not strong enough for universal testing.
- Other genetic predictors of treatment response: These are still being studied. For now, they help explain why one person responds differently than another more than they tell you exactly which drug will work best.
In other words, genetics may support a medicine decision, but it rarely makes the decision for you. The strongest use case is often medication matching, not diagnosis.
Broader overlap also deserves a careful read. Anxiety and depression can travel with IBS. Research into autism and shared genetic architecture is still emerging. Genetics should help reduce uncertainty, not label you or predict your symptoms on its own.
Your best next step is to bring genetics into the conversation when the picture is more complicated than usual. That includes severe symptoms, a strong family history, unusual features, or a treatment plan that may depend on CYP2D6 metabolism. A gastroenterologist or primary care clinician can help you decide whether genetic testing would add useful information.
A practical discussion works best when it stays anchored to the details that already matter most:
- What your symptoms look like now
- What seems to trigger them
- Which medicines have helped or caused problems
- Whether a genetic test could change a treatment choice
- Whether the result would actually change care
This content is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, and you should seek medical guidance for persistent, severe, or worsening symptoms. Results vary by person, and any dietary, supplement, or genetic advice should be individualized.
How Does IBS Overlap With Brain-Gut Health?

IBS does not sit in the gut alone. Genetic studies point to shared biology between digestive symptoms and brain-related traits, which is why gut-brain axis genetics matters for both body and mind. That overlap helps explain why anxiety, low mood, and IBS often show up together, even though IBS is still a digestive disorder. Genetic studies suggest that IBS shares inherited risk with several brain-related traits, especially depression and anxiety, while the overlap with inflammatory bowel disease appears minimal (source).
These findings do not mean IBS is a psychiatric disorder. They do suggest that neurogenetic pathways may shape how the brain, nerves, and immune system respond to stress and gut signals. In plain language, the same inherited risk can affect both bowel function and how strongly you feel worry, pain, or body sensations.
That pattern also shows up in clinical care. In one large genome-wide study, anxiety treatment was more common in IBS cases than in controls, which fits the broader brain-gut overlap seen in IBS research (source). The how stress affects IBS helps explain why stress can worsen pain, urgency, or bloating.
Hormonal shifts can matter too. hormones and IBS symptoms can be part of the picture when symptoms change with the menstrual cycle or other hormone changes.
Shared loci add another layer. In conditional false discovery rate analyses, researchers found overlapping genomic regions between IBS and brain-related traits. That means some variants may influence gut signaling and emotional regulation at the same time. The result is not one IBS gene. It is a network of shared risk across tissues and systems.
A quick way to think about it is this:
- Digestive side: bowel pattern changes, cramps, bloating, urgency, and food-related flares
- Brain side: anxiety, low mood, sleep disruption, and higher body sensitivity
- Shared biology: inherited risk that affects stress response and signaling in more than one system
For you, the practical takeaway is simple. If IBS shows up with anxiety, depression, panic, or other neuropsychiatric symptoms, treatment often works best when it addresses both sides of the loop. That may include gastrointestinal care, stress-focused strategies, psychological support, and other individualized options discussed with a qualified clinician. The goal is not to label symptoms as “all in your head.”
The goal is to treat a system that is clearly connected.
If your symptoms cross both categories, that pattern is worth bringing to a healthcare professional. A careful review can help sort out what needs gut treatment, what needs mental health support, and what may improve with both.
IBS Genetics FAQs
These IBS genetics FAQs address the questions people ask most often about family history, inherited risk, and what research can show so far. They can also help you organize your thoughts before talking with a healthcare professional.
1. Is There An IBS Genetic Test?
There isn’t a routine genetic test that can diagnose IBS, and most IBS genetics findings are still research-focused rather than clinically useful for everyone. A few studies have found SCN5A changes in a small subset of people with IBS, but that points to a possible clue, not a universal test. Pharmacogenomics IBS testing for CYP2D6 and CYP2C19 may help guide tricyclic antidepressant dosing, and it’s worth discussing if your clinician is considering that medicine or if your symptoms and family history raise concern about a broader inherited condition.
2. Can Twins Both Develop IBS?
Yes. Identical and fraternal twins can both develop IBS, which shows that genes are only part of the story. Twin studies have found heritability estimates from 0% in one British study to 57% in an Australian study, so the inherited signal looks real but uneven. For you and your family, the clearest takeaway is that IBS risk reflects both genetics and environment, including shared exposures, stress, and other life factors.
3. Is IBS Linked To Autism?
IBS may overlap with autism through broader brain-gut and neurogenetic pathways, but current evidence does not show a clear, direct genetic link. IBS is highly polygenic, and one study estimated about 12.1k ± 1.1k trait-influencing variants explain roughly 90% of its heritability, which points to many small effects rather than one autism-specific IBS gene. Shared genetic studies have found overlap with several psychiatric disorders, including 70 shared loci overall, but autism-focused research is still too small or mixed to tell whether any IBS-autism link is causal, indirect, or tied to overlapping symptoms and comorbidities.
4. Do Children Inherit IBS Risk?
Children can inherit a higher IBS risk, and family history matters because about half of people with IBS report another affected family member. First-degree relatives may have IBS two to three times more often than control relatives, and shared environment, including childhood antibiotics, can shape risk along with post-infectious IBS. In one large study, childhood antibiotic exposure appeared in 20.0% of IBS cases and 9.6% of controls, with an odds ratio of about 2.22, and family history raises awareness, not destiny. Regular meals, sleep, and stress support can help you spot recurring abdominal pain, bloating, constipation, or diarrhea early, and this content is for educational purposes only and is not a substitute for personalized medical advice.
Sources:
- http://creativecommons.org/licenses/by/4.0/: https://creativecommons.org/licenses/by/4.0
- PubMed: https://ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=16678561
- PubMed: https://ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=25649866
- PubMed: https://ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=27159638
- PubMed: https://ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=29184056
- PubMed: https://ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=29626450
- PubMed: https://ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=29700475
- PubMed: https://ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=31906708
- PubMed Central: https://ncbi.nlm.nih.gov/pmc/articles/PMC4321711
- PubMed Central: https://ncbi.nlm.nih.gov/pmc/articles/PMC5001845
