Visceral hypersensitivity in IBS guide explains why normal gut stretch can turn into pain, cramping, and urgency. Meals, bowel movements, or stress can make symptoms feel inconsistent, even when tests do not show structural damage. In plain language, it means the gut’s nerves react too strongly to ordinary signals, and the sections ahead show how to spot that pattern and respond with practical next steps.
The article breaks down peripheral versus central pain, the gut-brain axis, and the immune and nerve changes that can make IBS symptoms feel louder. It also covers sensory testing, low FODMAP trials, probiotics, neuromodulators, and when more labs or a gastroenterology referral make sense. Expect a practical framework for comparing patterns, tracking triggers, and choosing the next step without guesswork.
Adults with IBS, family caregivers, primary care teams, and gastroenterology clinicians will find the clearest value here because it connects symptom timing to treatment choice. A meal-linked bloating flare after a bowl of pasta, for example, points to a different path than pain that stays high even when the bowel is quiet. The next sections make the pattern easier to spot and the options easier to discuss.
Visceral Hypersensitivity in IBS Key Takeaways
- Visceral hypersensitivity means ordinary gut signals feel painful or urgent.
- IBS pain can reflect peripheral, central, or mixed sensitivity patterns.
- Meals, bloating, stooling, and stress can all intensify symptoms.
- Gut lining irritation, immune activity, and nerve signaling may all contribute.
- Low FODMAP trials help when symptoms are strongly meal-linked.
- Probiotics, neuromodulators, CBT, and TAVNS fit different IBS patterns.
- Blood in stool, weight loss, fever, or anemia need medical review.
What Is Visceral Hypersensitivity In IBS?

Visceral hypersensitivity in IBS means your gut feels pain too easily. Normal stretching, gas, or movement in the gastrointestinal tract can feel sharp, crampy, or unusually intense. In Irritable Bowel Syndrome (IBS), that makes visceral hypersensitivity a core part of the condition, not just an extra symptom.
It is one of the what causes IBS that helps explain why abdominal pain, bloating, cramping, and urgency can show up even when tests do not find structural damage. Clinicians commonly describe visceral hypersensitivity as an important feature of IBS, and studies have reported it in a substantial share of patients with the condition (source). That is why it gets considered across IBS subtypes when symptoms seem bigger than the test results.
In daily life, the pattern can feel inconsistent and hard to predict:
- After meals: Your belly may ache, swell, or feel tight after a normal portion of food.
- Around bowel movements: Cramping or urgency may rise before, during, or after a trip to the bathroom.
- During stress: Emotional strain can make gut symptoms feel louder and harder to ignore.
- With routine gut activity: Ordinary movement inside the bowel can trigger visceral pain that feels very real.
The pain is real. It is not “all in your head.” What changes is how the gut’s nerves read everyday signals, and that is where the gut-brain axis comes in. The gut and brain are in constant contact, so the same trigger may feel mild one day and severe the next.
That is also why symptom details matter so much in a medical visit. Describing the pain quality, where it sits, when it starts, and what seems to trigger it can help a clinician sort out a likely visceral hypersensitivity pattern from symptoms that need a closer look. Those details also make it easier to talk about meals, stress, and bowel habits without feeling brushed off.
Recognizing visceral hypersensitivity can make IBS feel less random and help guide your next steps. You may find it useful to track triggers, note symptom timing, and bring those patterns into conversations about diet or symptom-focused treatment. Persistent, severe, or worsening digestive symptoms still deserve review with a qualified healthcare professional.
Why Does The Gut Become So Sensitive?
Visceral hypersensitivity in IBS depends on the population and the test used (source). It means the nerves in your digestive tract react too strongly to normal stretch, gas, or movement. That is why everyday bowel activity can feel painful, urgent, or unusually intense, and why symptoms can seem to flare without a clear reason.
The main drivers usually fall into two broad groups:
Where the problem starts | What changes | What it can feel like |
|---|---|---|
Gut lining and immune activity | Mast cell activity, low-grade immune activation, epithelial barrier dysfunction, and higher intestinal permeability make the bowel wall easier to irritate | More pain, bloating, and discomfort from normal digestion |
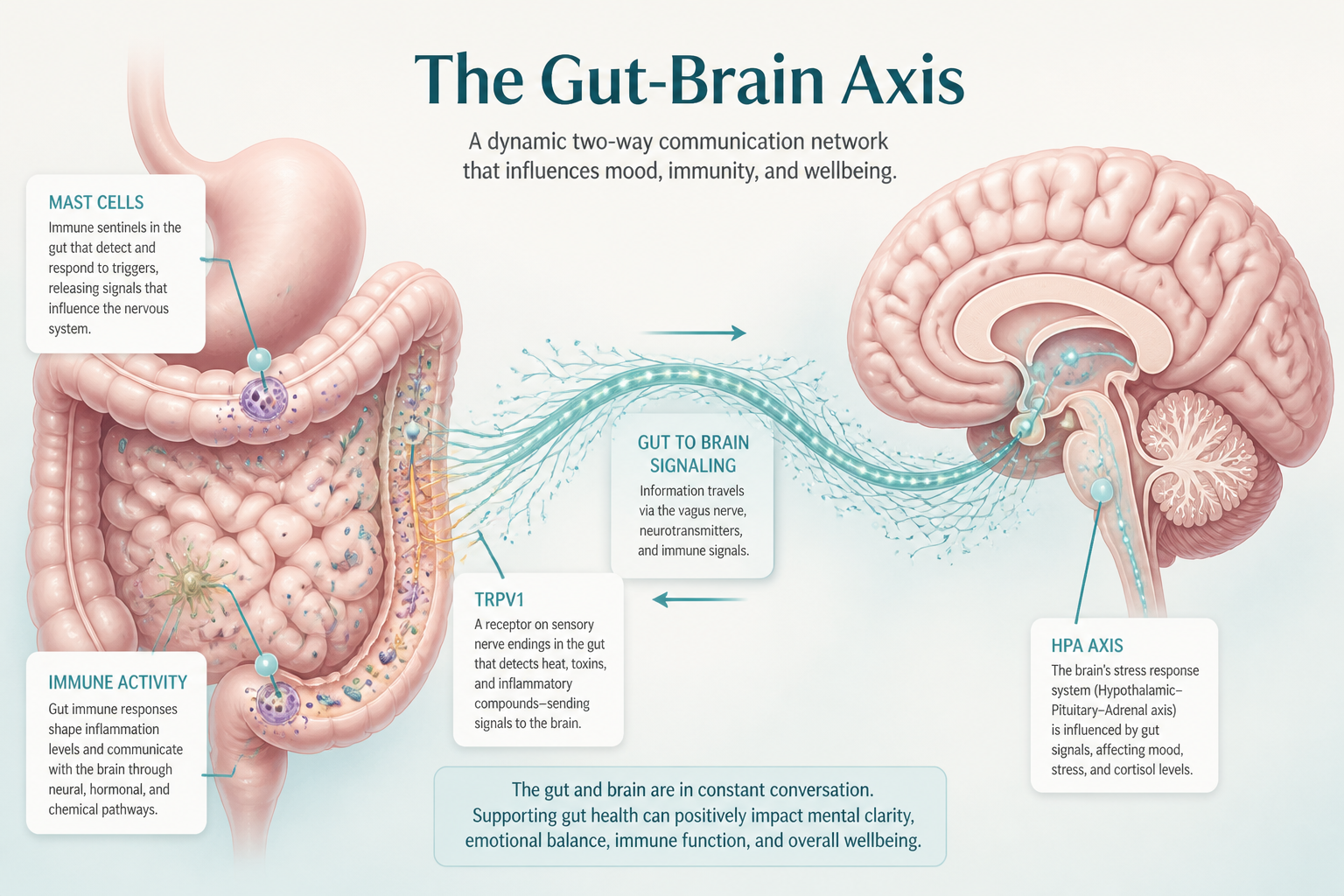
Nerve signaling in the gut | Research has linked visceral hypersensitivity in IBS to changes in pain-signaling pathways, including TRPV1, although the strength of the association varies across studies (source). | Mild signals feel sharp, urgent, or burning |
Brain and spinal processing | The gut-brain axis amplifies incoming signals from the bowel | The same stimulus feels stronger in IBS than in people without IBS |
On the gut side, a mast cell response can make the lining more reactive. Low-grade immune activation may also play a part, along with epithelial barrier dysfunction that weakens the gut’s usual protection. When intestinal permeability rises, the bowel wall becomes easier to irritate, and even normal stretching from gas or a bowel movement can feel excessive. Changes in gut motility in IBS can add to that pressure, since faster or slower movement changes how the bowel stretches.
Pain signaling can also become louder at the nerve level. TRPV1 helps nerves detect heat and irritation, and a more sensitive channel can let ordinary digestive activity cross into pain more easily. Once that threshold drops, your nervous system reacts to signals that would usually stay in the background. Other immune sensors may add to the response too, including Toll-like receptors (TLR4) and protease-activated receptors.
The gut does not work in isolation. The gut-brain axis carries signals in both directions, so the spinal cord and brain can turn up the volume on messages from the bowel. That central sensitization means the same stretch or cramp may feel mild in one person and very strong in another. Sometimes the signal is not bigger in the gut itself. Sometimes the processing system is louder.
Stress can raise that volume even more. The hypothalamic-pituitary-adrenal (HPA) axis is the body’s main stress-response system, and it can increase pain sensitivity, alter nerve signaling, and make symptoms feel more frequent during stressful periods. The hormones in IBS also matter here, because they can influence how strongly the HPA axis reacts and how steady your gut feels day to day. Stress does not create every symptom on its own, but it can make an already sensitive system much more reactive.
The plain-language takeaway is simple. IBS sensitivity usually comes from several overlapping changes at once. Gut lining irritation, immune activity, nerve signaling, and brain processing can reinforce one another over time, which is why symptoms often come and go and why layered management tends to work better than a single fix.
This content is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, so you should consult a qualified healthcare professional for persistent, severe, or worsening symptoms.
How Do You Phenotype Peripheral Vs Central Visceral Pain?
Visceral pain in IBS usually falls into two broad patterns, even though many people show a mix of both. Pain in IBS is often described as having peripheral and central components, and many patients show a mix of both rather than a single pattern (source). The goal is not a perfect label. It is matching your pattern to the treatment that is most likely to help.
Feature | Peripheral-dominant pattern | Central-dominant pattern |
|---|---|---|
Main driver | Sensitive bowel wall or gut trigger | Amplified pain processing |
Timing | Flares with meals, stooling, bloating, or bowel movement changes | More steady and less tied to eating or stooling |
Location | More localized or clearly linked to one area | More widespread or harder to pinpoint |
Other clues | Tenderness in a specific gut region, pain with bowel stress | Sleep disruption, anxiety, fatigue, or other functional pain syndromes |
Peripheral pain usually tracks with what the bowel is doing. Meals, bloating, stool changes, or a bowel movement can make it worse. It often feels localized, especially when stretch, irritation, or inflammation inside the bowel makes one area more reactive. TRPV1, a pain-sensing receptor in the gut, is one example of how a sensitive bowel wall can stay on alert.
Central pain looks different. It is often more widespread and less tied to eating or stooling. The pain may stay present between flares instead of showing up only during bowel activity. Sleep problems, anxiety, fatigue, migraine, pelvic pain, and other functional pain syndromes can travel with it, which suggests broader pain amplification rather than a single gut trigger.
The history and exam can add more shape to the picture:
- Focused tenderness: Pain reproduced when a clinician presses on one abdominal area can support peripheral or mixed sensitization.
- Bowel distension: Symptoms that flare when the bowel is stretched or distended also point toward a more gut-centered pattern.
- Generalized sensitivity: Strong reactions to many body sensations, not just gut sensations, can lean central.
- Pain out of proportion: Widespread tenderness without a matching local finding may suggest central sensitization.
No single finding sorts this out on its own. The full pattern matters more than one isolated clue.
Experimental pain tests such as thermal, ischemic, and cold pressor testing are used in research to study pain sensitivity, but they are not routine office tests for IBS (source). These measures can show overlap between visceral and somatic hypersensitivity in IBS, which helps explain why one treatment rarely fits everyone. They can also hint at whether your pain is mostly gut-driven, more centrally amplified, or mixed.
That difference matters when you choose treatment. Central-dominant pain may respond better to therapies that target pain processing, while gut-focused treatments may fit better when symptoms are clearly bowel-related (source). The vagus nerve is part of that conversation because it helps carry signals between the gut and brain. In some cases, transcutaneous vagal stimulation (TAVNS) is discussed as one possible tool alongside other non-drug or medication options.
Mixed patterns are common, so this framework works best as a guide rather than a rigid diagnosis. Combine what you feel, what the exam shows, and any testing that is available, then adjust the plan based on the dominant pattern. If pain is severe, persistent, or hard to explain, specialist evaluation can help sort out the next step without assuming one mechanism explains everything.
Which Features Suggest Peripheral Pain?
Peripheral-dominant pain often feels tied to the gut itself rather than spread across the whole body. The pattern is usually repeatable, meal-linked, and easier to localize during an exam, so the story your symptoms tell matters.
Look for these bedside clues:
- Post-infectious onset: Symptoms that begin after a stomach bug, food poisoning, or another clear GI trigger can fit a gut-sensitized pattern. Post-infectious IBS is one example of how an infection can leave sensory nerves on high alert.
- Meal-linked flares: Pain that worsens after meals, certain carbohydrates, alcohol, or the same repeat trigger often points toward peripheral visceral pain. When eating sets off symptoms more often than stress or worry, food triggers in IBS may be part of the picture.
- Focal tenderness: Pain that keeps returning to one spot, such as a tender area in the lower abdomen, is another clue. Localized tenderness during a bedside exam often fits better than pain that feels diffuse or hard to pin down.
- Gut activity patterns: Cramping, urgency, bloating, and diarrhea that rise and fall with bowel activity support a gut-driven source. Reproducible symptoms tied to meals and abdominal tenderness matter more than body-wide pain without a clear abdominal pattern.
- Immune and nerve signals: Flushing, itching, hives, nasal symptoms, or several food sensitivities can point to mast cell activity. Research has linked visceral hypersensitivity in IBS to several immune and pain-signaling pathways, including prostaglandin signaling and receptor activity, but the exact mechanisms are still being studied (source).
Curcumin and berberine belong in the symptom-support bucket, not the diagnosis bucket. They may fit into a broader plan, but they do not show you where the pain starts.
These clues do not diagnose the problem by themselves. They suggest that the bowel wall and its nerves may be doing more of the talking, which can help you describe symptoms to a clinician and decide whether more evaluation is needed. This content is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, and persistent, severe, or worsening pain deserves medical review.
Results vary by person, and any dietary or supplement advice should be individualized.
Which Tests Guide The Match?
The most useful IBS tests answer a narrow question.
A standard clinical evaluation still comes first. Your symptom pattern, physical exam, and alarm-feature review help decide whether pain fits IBS-related visceral hypersensitivity or points to another cause that needs more workup. That order matters because the test should match the clinical question.
A quick map of the main options looks like this:
Test type | What it can show | How it fits care |
|---|---|---|
Rectal distension threshold testing | How much stretch the rectum tolerates before pain starts | Helps phenotype sensitivity, but mostly stays in research |
Barostat-style sensory testing | Pressure and stretch responses in the rectum | A form of experimental pain testing, not routine office care |
Blood work and stool tests | Signs of inflammation, infection, or anemia | Helps rule out other conditions when symptoms warrant it |
Breath testing | Carbohydrate malabsorption or small intestinal bacterial overgrowth (SIBO) | Useful when bloating, gas, and post-meal pain suggest a trigger |
Validated questionnaires and pain scales | Severity, stool pattern, bloating, and food links over time | Good bedside tools for tracking phenotype and treatment response |
Rectal distension and barostat-style sensory tests are used to study visceral sensitivity, but they are mainly research tools and are not part of routine IBS care (source).
Basic labs and stool studies do not diagnose visceral hypersensitivity directly. They can still support a more confident IBS diagnosis by helping rule out inflammation, infection, or anemia. Breath testing may help when symptoms suggest carbohydrate malabsorption or small intestinal bacterial overgrowth, especially when bloating and pain follow meals (source).
That branch matters even more when methane and Methanobrevibacter smithii seem likely, because treatment choices may shift if fermentation or slow transit is part of the picture. In some cases, that changes the conversation around diet, antibiotics, or probiotics. Validated questionnaires also help you track symptoms over time, even though they do not measure sensitivity as precisely as specialized sensory tests.
Researchers are still studying biomarkers and better ways to sort IBS phenotypes, and updates continue to appear through sources such as the NCBI RSS feed (NCBI RSS feed). For now, the best match is the simplest test that answers the question in front of you, with bedside tools guiding everyday decisions and specialized testing staying mostly in the research lane.
Which Treatments Help Most, And For Whom?

Which treatment helps most depends on whether your pain looks more peripheral or central.
Treatment choice in IBS often depends on whether symptoms are more meal-linked and bowel-related or more stress-sensitive and widespread, because patients can differ in how pain is driven and experienced (source).
A simple way to compare options is to match the treatment to the pattern:
Treatment | Best fit | What it tends to help | Practical notes |
|---|---|---|---|
low FODMAP diet | Meal-linked symptoms, bloating, distension, and pain after eating | Gas, stretch pain, and food-triggered flares | Best as a short, guided trial with reintroduction so you can find personal triggers |
probiotics | IBS-D, mixed bowel habits, and prominent bloating | Abdominal pain and bloating, with modest and variable benefit | Strain choice matters, and longer trials usually make more sense than very short ones |
Neuromodulators and cognitive behavioral therapy | Central-dominant pain, sleep disruption, anxiety, or hypervigilance | Pain signaling and stress amplification | These work over weeks, not hours, and side effects can shape the choice |
Mast-cell, anti-inflammatory, anti-secretory, and plant-derived options | Food-triggered symptoms, inflammatory flares, or post-infectious IBS | Pain, bloating, and diarrhea in selected patients | Curcumin, berberine, peppermint oil, fennel combinations, and crofelemer may fit here |
neuromodulation | Persistent symptoms despite standard care, especially mixed bowel symptoms or a strong peripheral component | Pain and bowel symptoms in selected cases | Benefits may take several weeks, and access is still limited |
Diet-based therapy usually comes first when symptoms flare after meals. A structured low FODMAP diet trial may help some people with IBS when symptoms are meal-related and bloating is prominent, especially when the plan includes reintroduction to identify personal triggers (source). Keep the trial short, then bring foods back one group at a time so you learn what actually bothers you instead of staying restricted longer than needed.
The goal is not to avoid everything. The goal is to find the foods that matter most, then widen your diet as much as you can tolerate.
Microbiome-directed therapy is another symptom-targeted tool, not a universal fix. Probiotics may help by shifting the gut microbiota, but results depend on the strain, the dose, and how long you use it. Some probiotic studies have reported improvements in pain and bloating for selected IBS patients, but the benefit depends on the strain, dose, and treatment length (source).
The benefits are usually modest. People with IBS-D, mixed bowel habits, or stubborn bloating are often the best match, but even then the response can vary a lot from one product to the next.
When pain feels central, brain-gut pain treatments make more sense than more diet changes. That is where neuromodulators and cognitive behavioral therapy can help, especially if pain is frequent, stress-reactive, sleep-disrupting, or paired with anxiety and body scanning. These approaches lower pain signaling over time, so they are aimed at weeks of change rather than immediate relief, and side effects like sedation, constipation, and dry mouth often guide the dose and the drug choice.
A few other options fit better when the story points toward inflammation, immune activation, or secretory diarrhea. Curcumin, berberine, peppermint oil, and fennel combinations may ease pain and bloating in selected people, especially after an infection or during food-triggered flares. Crofelemer also belongs in this group because it reduces fluid secretion in the bowel.
A small trial in women with IBS-D reported symptom improvement with crofelemer 125 milligrams twice daily, but the evidence remains limited and should be interpreted cautiously (source).
For symptoms that keep going despite standard care, neuromodulation is worth knowing about. One emerging option is TAVNS, which works through the vagus nerve and is still not widely available. A randomized study in IBS-C reported symptom improvement with transcutaneous auricular vagal nerve stimulation, but the evidence is still early and the therapy is not widely available (source).
A simple way to think about your next step is this:
- Meal-linked, bloating-heavy symptoms: start with a guided low FODMAP diet trial.
- Bloating plus loose stools or mixed bowel habits: consider strain-specific probiotics and a review of your gut microbiota strategy.
- Pain that tracks with stress, sleep loss, or fear of symptoms: ask about neuromodulators and cognitive behavioral therapy.
- Inflammatory or post-infectious flare patterns: discuss anti-secretory, anti-inflammatory, and plant-derived options.
- Persistent symptoms after standard care: ask whether TAVNS or another form of neuromodulation is realistic for you.
Digestive symptoms can have many causes, so persistent, severe, or worsening symptoms deserve medical evaluation. This content is for educational purposes only and is not a substitute for personalized medical advice. Results vary by person, and diet, probiotic, or supplement choices should be individualized with a clinician who knows your full history.
When Should You Seek More Testing Or Referral?
More testing makes sense when your symptoms stop fitting a usual IBS pattern. The goal is not to dismiss your pain. It is to make sure another treatable condition is not being missed before visceral hypersensitivity is assumed.
Signs that deserve medical review include:
- Blood in the stool
- Unexplained weight loss
- Fever
- Persistent vomiting
- Anemia
- Nighttime symptoms that wake you up
- A strong family history of inflammatory bowel disease or colorectal cancer
A new pain pattern, repeated acute flare-ups, or bowel changes that do not match your usual rhythm deserve a broader workup. Family history can matter too, and IBS genetics may help explain risk, but it should never be used to brush past red flags.
Referral is often appropriate when symptoms stay persistent, severe, or worse despite reasonable first-line care. That usually means diet changes, stress management, and other IBS treatments have already been tried. Ongoing or concerning digestive symptoms deserve medical review, especially when they include blood in the stool, weight loss, fever, persistent vomiting, anemia, or nighttime symptoms that wake you up (source).
Common next steps often look like this:
Test | What it helps rule out |
|---|---|
Blood work | Anemia, inflammation, and other signs of systemic illness |
Stool tests | Infection or intestinal inflammation |
Celiac testing | Celiac disease |
Imaging or other studies | Structural or anatomical problems |
Clinicians usually look for alarm features and may order blood tests, stool tests, celiac testing, or other studies to rule out conditions that can mimic IBS (source). IBS is usually diagnosed after those conditions have been considered. Specialized visceral pain threshold tests, including thermal, ischemic, and cold pressor studies, can show overlap between visceral and somatic hypersensitivity in research settings, but they are not part of routine day-to-day diagnosis.
A simple next-step workflow can keep the process clear:
- Track your symptoms, meal triggers, and flare patterns for a short, focused period.
- Bring a concise history to your clinician, including what has changed and what feels new.
- Ask which serious causes still need to be excluded.
- Follow through with labs, stool tests, imaging, or gastroenterology referral if they are recommended.
- Keep an open mind about other possibilities. Fecal microbiota transplantation belongs in specialist care or research settings, not in a routine IBS workup.
More testing is a safeguard, not a verdict. It helps avoid missing another treatable condition while still respecting that IBS pain can be real even when standard tests come back normal. This content is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, and persistent, severe, or worsening symptoms deserve evaluation from a qualified healthcare professional. Results vary by person, and any next steps should be individualized.
Visceral Hypersensitivity In IBS FAQs
These FAQs cover the questions you may have about visceral hypersensitivity in IBS, including why everyday gut signals can feel intense and how symptoms may relate to meals, stress, and care choices. They’re here to help you make sense of what’s happening before you think about treatment.
1. Is Visceral Hypersensitivity The Same As IBS?
No, visceral hypersensitivity is not the same as IBS. It is one key way IBS can trigger stronger abdominal pain and cramping, because your gut may register pain at lower-than-usual levels. IBS also includes bowel habit changes and other drivers, so you can have a sensitive gut without IBS, or have IBS shaped by more than one factor.
2. Can Stress Worsen Visceral Pain In IBS?
Stress can make IBS pain feel louder because your brain and gut read normal signals differently when pressure is high. The IBS stress link explains how HPA-axis shifts, including cortisol changes, can raise pain sensitivity and make you more reactive to bowel activity. CRH signaling, especially through CRH1 pathways, is another likely mechanism, which helps explain why stress can amplify both visceral pain and motility changes.
3. Do Low-FODMAP Diets Help Visceral Hypersensitivity?
A low FODMAP diet can ease IBS symptoms for some people because it cuts back on poorly absorbed carbs that can create gas and draw water into the gut, which may reduce pain triggers tied to visceral hypersensitivity. The evidence is supportive but not universal, so it can help some people without helping everyone, and it is not a cure. A short 4 to 6 week trial with a registered dietitian, followed by careful reintroduction, is often best when your pain feels meal-related, bloating stands out, or you want to avoid long-term restriction, and you should discuss persistent, severe, or worsening symptoms with a qualified healthcare professional.
4. Can Visceral Hypersensitivity Improve Over Time?
Yes, visceral hypersensitivity can improve over time, especially when you treat the IBS drivers instead of trying to ignore the pain. Progress is usually gradual, and it’s more likely when diet changes, IBS medications, stress management, cognitive behavioral therapy, hypnotherapy, and biofeedback help calm pain signaling and reduce triggers. Your symptom pattern matters too, and if symptoms stay severe or keep changing, you should talk with a qualified healthcare professional because digestive symptoms can have many causes and results vary by person.
Sources:
- https://creativecommons.org/licenses/by/4.0/: https://creativecommons.org/licenses/by/4.0
- HHS: https://hhs.gov/
