IBS and gluten often get linked, but the real picture is usually more complicated. Many adults with IBS notice bloating, pain, gas, or bowel changes after bread or pasta, then wonder whether gluten, wheat fructans, or celiac disease is behind it. Clear next steps matter here because guessing can delay the right test and push food restriction farther than it needs to go.
IBS is a functional gut disorder, which means symptoms are real even when scans and standard tests look normal. This article covers how to tell IBS from celiac disease, when NCGS enters the picture, and how FODMAPs and fructans can mimic a gluten problem. It also lays out the order of testing, the role of a dietitian-guided food trial, and the signs that make medical evaluation the safer move.
For adults and families managing digestive symptoms, the goal is not just symptom relief but a clearer food plan that fits daily life. A reader who feels worse after a gluten-free switch may learn that the trigger was wheat fructans, not gluten itself, and that celiac testing should have happened first. My Good Gut keeps the path practical, so the next steps stay evidence-informed, manageable, and medically sound.
IBS and Gluten Key Takeaways
- IBS symptoms can overlap with wheat, gluten, and fructan reactions.
- Celiac disease must be tested before long-term gluten removal.
- NCGS can mimic IBS, but it is a diagnosis of exclusion.
- Fructans in wheat often cause bloating and gas.
- Low FODMAP diets often identify triggers better than gluten-free diets.
- Dietitian-guided reintroduction helps separate gluten from other food triggers.
- Red flags like weight loss or anemia need medical evaluation.
How Are IBS And Gluten Connected?

Irritable bowel syndrome (IBS) is a functional gut disorder, and food choices sit at the center of your IBS eating plan. That means tests can look normal even when your gut reacts strongly to certain foods, stress, and routine changes. If you live with IBS, abdominal pain, bloating and gas, diarrhea, constipation, or mixed bowel habits can still flare without structural damage.
The overlap with wheat is where things get messy. Wheat, rye, and barley contain both gluten and fructans, and IBS trigger foods to limit often removes those foods for more than one reason. Fructans are short-chain fermentable carbohydrates. They are poorly absorbed in the small intestine, then move into the colon, where gut bacteria break them down fast.
That process can produce extra gas and pull water into the bowel. In IBS, that pressure can stretch the bowel wall and lead to bloating, cramping, urgency, diarrhea, or constipation. A bread-heavy meal may feel like proof that gluten is the problem, but wheat fructans are often the more likely trigger.
Gluten gets blamed because cutting bread, pasta, crackers, and baked goods removes both gluten and fructans at the same time. If you feel better after going gluten-free, that improvement does not prove gluten was the only issue. It may also reflect lower fiber intake, changes in meal patterns, or expectation effects.
The research points in that direction too. Reviews of the literature suggest that self-reported wheat or gluten sensitivity is common, while true gluten-specific reactions appear less common (source). Other wheat compounds, fructans, lower fiber intake, and the placebo or nocebo effect explain many cases.
A smarter next step is to sort out the trigger instead of guessing:
- Test for Celiac Disease first: this should happen before you remove gluten long term.
- Try a dietitian-guided low FODMAP plan: this can help show whether fructans are behind your symptoms.
- Reintroduce foods one group at a time: this helps separate gluten from other triggers.
- Track symptoms clearly: note bloating, gas, stool changes, and meal timing.
This gives you a clearer path when food triggers IBS symptoms, and it helps you make choices that actually fit your body.
How Do You Tell IBS From Celiac Disease?
The core difference is straightforward. Celiac disease is an autoimmune condition in which gluten damages the small intestine, and treatment requires a lifelong strict gluten-free diet. IBS is a functional disorder, so the diagnosis of IBS usually comes from symptom patterns and the Rome criteria after other causes are considered.
The tests that separate the two are different:
- Celiac disease: A celiac blood test usually starts with tissue transglutaminase IgA, plus total IgA. A small bowel biopsy may follow if results are unclear or a specialist wants confirmation.
- IBS: No single test proves IBS. Clinicians usually look for symptom patterns and test for celiac disease, inflammatory bowel disease, or other warning signs instead.
Timing matters a lot for celiac testing. If you stop gluten before bloodwork or biopsy, antibody levels can fall and the results can miss the condition. That can create false negatives in both serology and biopsy. If celiac disease is on your radar, keep eating gluten until a qualified healthcare professional tells you to stop.
Certain features make celiac disease more suspicious than IBS:
- Chronic diarrhea
- Unintentional weight loss
- Iron-deficiency anemia
- Fatigue
- Nutrient deficiencies
- Family history of celiac disease
Bloating, abdominal pain, and bowel changes can happen in both conditions, so symptoms alone are not enough. Celiac disease and IBS can also coexist. Feeling better on a gluten-free diet does not prove celiac disease, because some people react to wheat fructans or other fermentable carbohydrates instead of gluten itself.
That's where non-celiac gluten sensitivity can confuse the picture. NCGS can overlap with IBS symptoms, but it is not the same as celiac disease.
Situation | What it often means |
|---|---|
Diarrhea-predominant or mixed IBS | Celiac screening is often appropriate |
Positive blood test | A specialist may recommend biopsy |
Negative testing after gluten restriction | Results may be unreliable |
Studies show that celiac disease is more common in people who meet IBS criteria than in control groups, so celiac testing is often recommended when IBS symptoms overlap with celiac symptoms (source, source). If celiac disease is a possibility, talk with a qualified healthcare professional before starting or restarting a gluten-free diet so testing happens while you are still eating gluten.
How Do You Test Gluten Vs Fructans?
The safest way to sort out Gluten vs Fructans is to rule out celiac disease first. If celiac is still possible, you need to stay on a gluten-containing diet long enough for blood tests, and sometimes a biopsy, to stay accurate. Stopping gluten too early can lower antibody levels and create a false-negative result.
Wheat allergy belongs in the differential when the pattern looks allergic. It is an immunoglobulin E, or IgE, mediated reaction to wheat proteins, not celiac disease or non-celiac gluten sensitivity. Hives, swelling, wheezing, or a rapid severe reaction point toward allergy testing instead of a food-intolerance trial.
Wheat can be hard to read on its own because it carries more than one trigger. Rye and barley matter too, but wheat also removes both gluten and wheat fructans at the same time. Feeling better after going wheat-free does not prove the problem is gluten. It may be the fermentable carbohydrate.
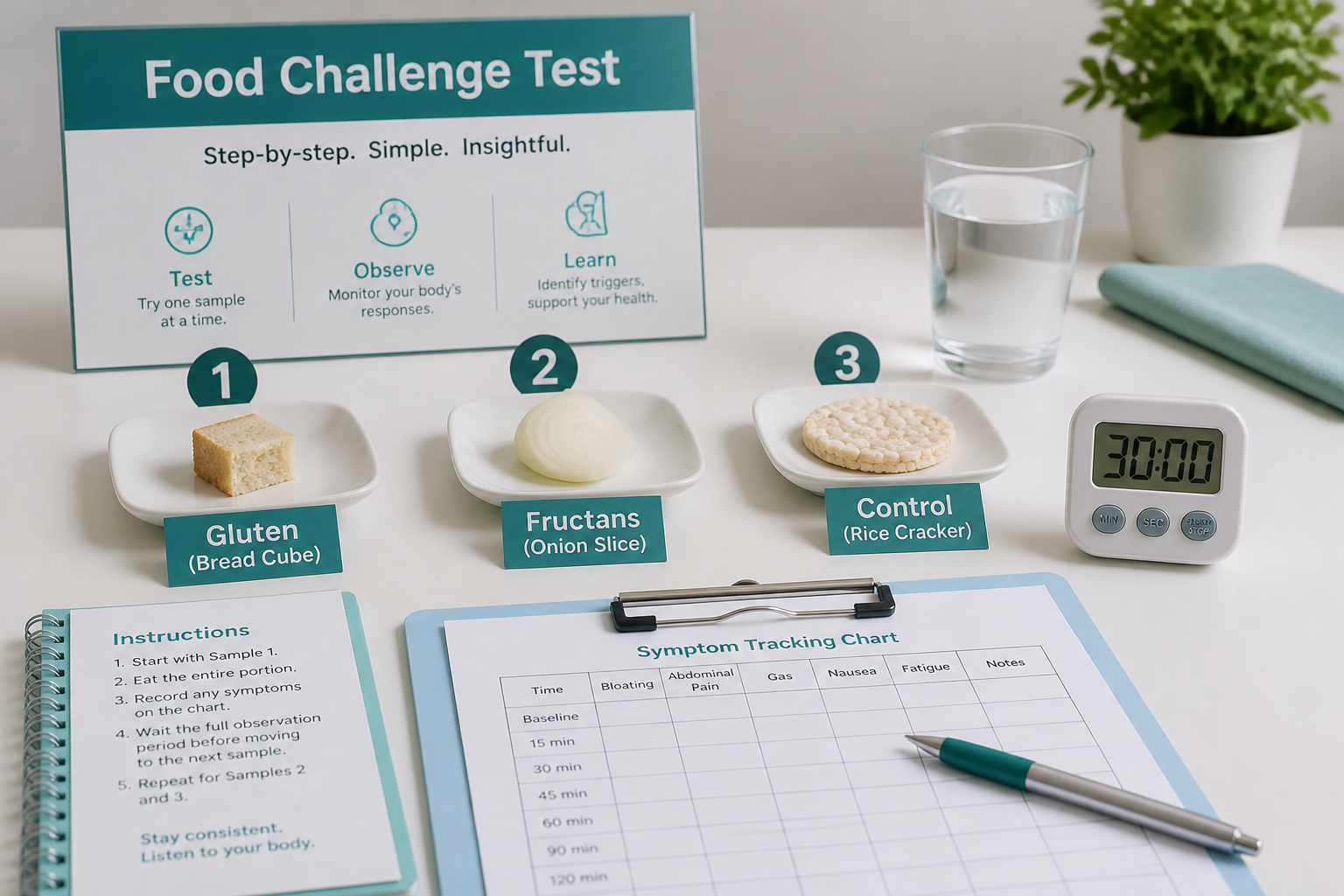
A structured gluten challenge helps separate those possibilities. The Salerno criteria use controlled exposure to reduce guesswork, and the same logic works in everyday care:
- Establish a stable symptom baseline first.
- Test one exposure at a time.
- Compare gluten, fructans, and a control.
- Track symptoms the same way after each challenge.
Blinded challenge studies in adults with IBS suggest that gluten alone does not trigger symptoms for many people, and some symptoms may be driven by other wheat components such as fructans (source). A low-FODMAP plan can help because FODMAPs include the fructans that often ride along with wheat. Many dietitians use low-FODMAP reintroduction to isolate wheat fructans more cleanly than wheat avoidance alone.
The comparison is simple:
Test focus | What it helps you learn |
|---|---|
Gluten | Whether the protein tracks symptoms |
Fructans | Whether fermentable carbs are the main issue |
Control | Whether symptoms are from the challenge or normal day-to-day variation |
Dietitian-guided interpretation matters because adherence can be messy. Studies that checked compliance found that many people did not eat the intended test bars, which can blur the result and make a trigger look stronger than it is. Results vary by person, and the most useful test plan stays structured, documented, and medically guided.
Is Gluten-Free Or Low FODMAP Better For IBS?
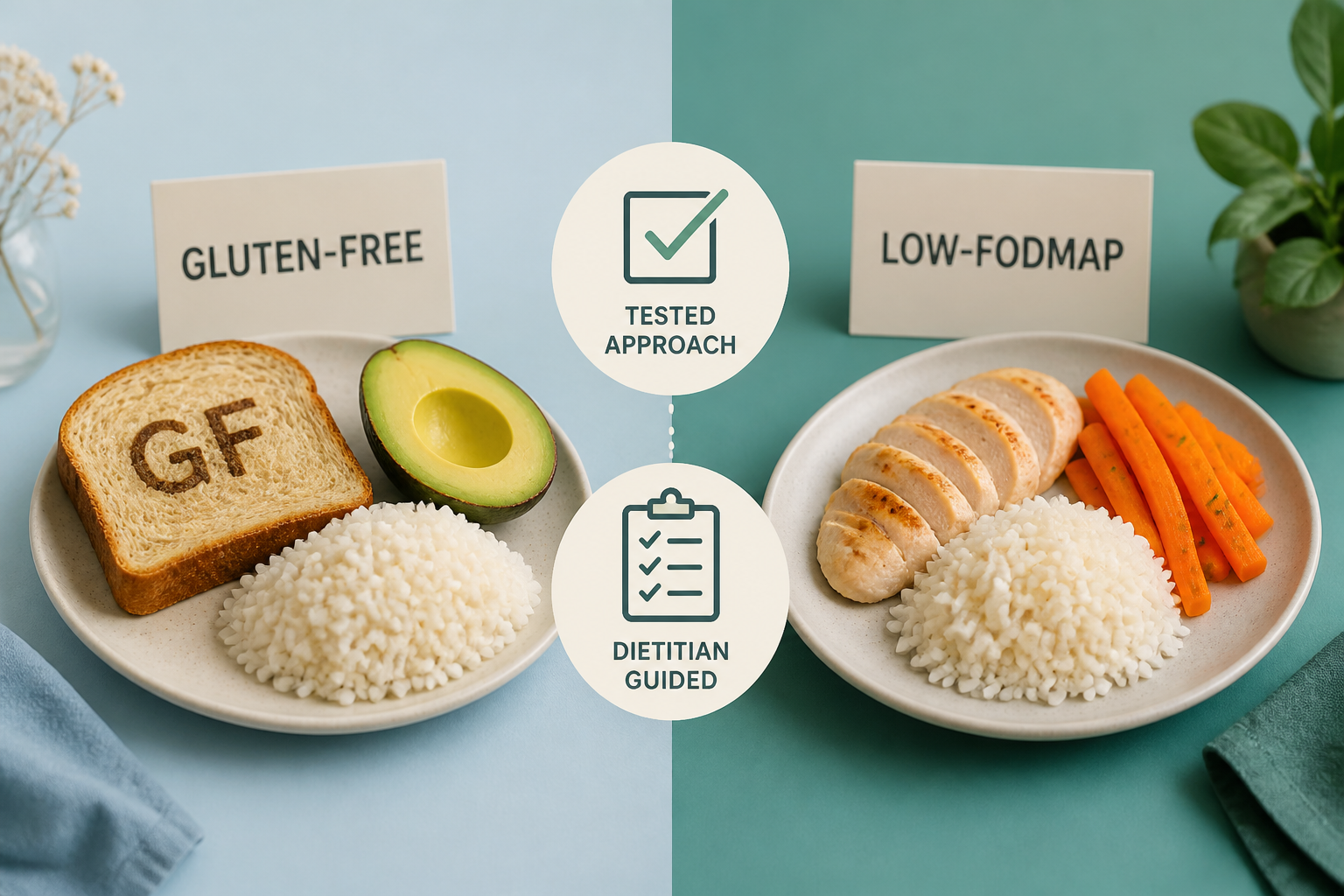
For many people with IBS, a low FODMAP diet can be a useful first step because it targets fermentable carbohydrates such as fructans instead of focusing only on gluten (source, source). Those carbs are common in wheat, which is why bread or pasta can seem to be the problem when the real trigger may be the FODMAPs instead of gluten itself.
A low-FODMAP foods for IBS is often more useful than a plain gluten-free diet for spotting patterns. A dietitian supervised low FODMAP plan keeps the process structured and makes symptom reintroduction easier after the short elimination phase. That stepwise method is also reflected in the Monash University FODMAP Diet and NIDDK guidance.
A gluten-free diet can still be a reasonable place to start if you want something simpler and less restrictive. It may help when wheat-based foods seem tied to bloating, pain, or bowel changes. The downside is that it can miss other triggers, and it does not show whether fructans, another FODMAP, or a different food is driving your symptoms.
The trade-offs look like this:
Approach | What it tests | What you may notice | Main trade-off |
|---|---|---|---|
Gluten-free diet | Wheat and gluten-containing foods | Changes may show up within a few weeks | It can stay restrictive and may lower fiber or key nutrients if replacements are poor |
Low FODMAP diet | Multiple fermentable carbs, including fructans | Relief often appears during the short elimination phase | It is more complex at first, but better for identifying the true trigger |
For most people with IBS, the bigger long-term win is not just short-term relief. It is learning what you can eat comfortably without cutting out more than you need.
Working with a registered dietitian who specializes in gastrointestinal health can make that process safer and easier. Good support helps you stay nutritionally adequate, avoid over-restriction, and use symptom reintroduction to separate true triggers from foods you can likely tolerate.
How Do You Avoid Over-Restricting Your Diet?
The safest way to avoid over-restricting your diet is to test first, then cut back only as long as needed. If you have unexplained weight loss, iron-deficiency anemia, persistent diarrhea, blood in the stool, severe symptoms, or a family history of celiac disease, get medical evaluation before making changes. Keep eating gluten until celiac testing is complete so the result stays accurate.
A gluten-free diet is not always the first or only step. For some people, a short gluten elimination helps because it also lowers wheat fructans, which are a type of FODMAP. For others, especially when more than one food seems to set off symptoms, the best IBS diet may look more like a dietitian supervised low FODMAP plan than a strict gluten-free diet.
Time limits matter, too. A short elimination phase gives you useful data without trapping you in long-term restriction. Some people notice changes in a few days, while others need a few weeks. The goal is symptom reintroduction, so you can sort out gluten, fructans, and wheat from the rest of your food triggers IBS.
A registered dietitian with GI experience can help you keep meals balanced, compare gluten-free and low FODMAP choices, catch accidental gluten exposure, and make sense of mixed symptoms without turning food into a permanent fear list.
A simple decision-tree toolkit can keep you on track:
- Rule out celiac disease first.
- Check for wheat allergy and other IBS triggers.
- Choose the least restrictive trial that fits your symptoms.
- Track meals and symptoms briefly.
- Refer to a clinician or gastroenterologist if symptoms are severe, worsening, or come with alarm signs.
This approach protects the diagnosis of IBS from guesswork and keeps your next step focused, practical, and safe.
IBS and Gluten FAQs
These FAQs focus on the questions that come up when IBS and gluten seem connected, especially how to tell true triggers from common mix-ups. They also reference the Monash University FODMAP Diet and the NIDDK IBS Diet Guidelines so you can compare your options with more confidence.
1. Why Does Gluten Trigger IBS Symptoms?
A lot of “gluten” trouble in IBS may actually come from wheat fructans, which gut bacteria ferment into gas that can stretch the bowel wall and drive bloating and gas like cramping and bowel changes without causing damage. If gluten protein is the real issue outside celiac disease, researchers think it may involve a mild innate immune response or a microbiome shift rather than the autoimmune injury seen in celiac disease, and IBS and grains covers that overlap in more detail. Wheat amylase-trypsin inhibitors are another possible trigger because they may irritate the gut and affect motility, which can leave you feeling more urgent, crampy, and swollen even when the intestine isn’t being harmed.
2. Can Wheat Cause IBS Without Gluten?
Yes. Wheat can trigger IBS symptoms even when gluten is not the main issue because it also contains fructans, a type of FODMAP that can add to symptoms. That fermentation can cause bloating, gas, abdominal pain, and bowel changes, and other wheat compounds such as wheat amylase-trypsin inhibitors may bother your gut too. A wheat reaction does not automatically mean celiac disease or gluten is the cause, so talk with a healthcare professional before removing several foods for the long term.
3. Is Non-Celiac Gluten Sensitivity Real?
Yes, non-celiac gluten sensitivity (NCGS) is a real clinical label, but it’s a diagnosis of exclusion after celiac disease and wheat allergy are ruled out. It does not cause the intestinal damage seen in celiac disease, and its exact mechanism is still unclear, though symptoms can include bloating, pain, fatigue, headaches, brain fog, and possible changes in intestinal permeability. Blinded challenge studies show that pure gluten does not trigger symptoms in most people with IBS, so a gluten-free response may reflect FODMAPs like wheat fructans, expectation effects, or other factors rather than gluten itself.
4. How Long Should A Gluten Trial Last?
If you haven’t had celiac disease testing yet, stay on gluten and get evaluated first, because starting a gluten elimination too early can distort blood tests and biopsies. For a supervised symptom trial, give yourself at least 30 days, then do a gradual gluten challenge by starting with a small serving and increasing to a normal serving over several days while you track pain, bloating, stool changes, and energy. The Salerno criteria place more weight on a clear pattern of improvement off gluten and symptom return with reintroduction than on a one-day reaction, and if you have red flags like weight loss, iron-deficiency anemia, blood in the stool, persistent diarrhea, or a family history of celiac disease, test first and talk with your doctor.
