Hormones in IBS affect symptom patterns, bowel speed, and pain sensitivity. For people whose bloating, constipation, diarrhea, or cramping changes around a period or midlife hormone shifts, the pattern can look random until the timing is mapped. In plain terms, hormones in IBS are symptom shapers more than a single root cause. The result is a clearer way to track when symptoms rise, what they look like, and when HRT or contraception deserves a closer look.
Key topics include estrogen, progesterone, testosterone, cortisol, the HPA axis, and the microgenderome, along with menstrual cycle flares, perimenopause, menopause, stool patterns, and HRT timing. The seven takeaways at the end turn that into a symptom log, a Bristol stool check, and a short list of when to ask about HRT or contraceptives. They also flag the pain, stool changes, and cycle patterns that deserve medical review.
Adults living with IBS, especially menstruating, perimenopausal, and menopausal women, along with caregivers and generalist clinicians, get the most value here. A monthly log that links cramps, bloating, and Bristol type 7 stool to the luteal phase can separate hormone-linked flares from food reactions. The next sections offer a practical way to make those patterns easier to act on.
Hormones in IBS Key Takeaways
- Estrogen, progesterone, testosterone, cortisol, and microbes can shape IBS symptoms.
- Estrogen may heighten pain, bloating, and urgency during hormone swings.
- Progesterone often slows transit and can push symptoms toward constipation.
- Menstrual, perimenopausal, and menopausal shifts can change symptom timing.
- Bristol stool tracking helps connect stool form with hormone-related flares.
- New symptoms after HRT or contraceptives should be discussed with a clinician.
- Symptom logs and stress care help match treatment to flare timing.
Which Hormones Are Linked to IBS?

Hormones in IBS are better seen as symptom shapers than as a single root cause. The idea behind hormones in IBS is that shifts in pain, bowel speed, and gut sensitivity often happen together. That pattern fits factors behind IBS, where several body systems overlap instead of one issue explaining everything.
Estrogen often sits at the center of the conversation. The link between estrogen and irritable bowel syndrome is easiest to spot when symptoms start or worsen after puberty and sometimes ease after menopause. Estrogen can affect gut barrier integrity, mucosal immunity, mast cell activity, and visceral sensitivity, which helps explain bloating, pain, and cycle-linked flares.
A quick map of sex hormones in IBS helps:
Hormone or system | What it may do in the gut | IBS pattern it may fit |
|---|---|---|
Estrogen | May shift barrier function, immune signaling, mast cell activity, and pain sensitivity | Bloating, cramping, and flares that track the menstrual cycle |
Progesterone | May slow gut motility and make stools harder | IBS-C, constipation, and a slowed-digestion feeling |
Testosterone | May calm stress reactivity and inflammatory signaling | Lower pain tolerance and more mixed symptoms in some people |
Cortisol and the HPA axis | May intensify gut-brain signaling and pain sensitivity | Stress-sensitive flares, IBS-M, and anxiety-linked worsening |
Microgenderome | May reflect the two-way influence between hormones and microbes | Diarrhea, constipation, pain, and cycle-related changes |
Progesterone is a common clue when constipation is the main pattern. Levels rise in the luteal phase, which is the stretch after ovulation and before your period, and they also rise in pregnancy-like hormonal states. That can slow motility, harden stools, and leave you feeling backed up.
Testosterone is discussed less often, but it may still matter. Lower levels may be linked with stronger stress responses, more pro-inflammatory signaling, and greater visceral pain sensitivity. That can help explain why IBS patterns can look different between sexes even when the day-to-day symptoms seem similar.
Cortisol and the hypothalamic-pituitary-adrenal (HPA) axis matter too. This stress system can turn up gut-brain signaling and make bowel habits less predictable, which is why the stress and IBS flares is such a big part of the picture. Ongoing anxiety, poor sleep, or physical stress can make mixed bowel patterns more noticeable and keep flares going longer.
The other piece is the microgenderome, which describes the two-way relationship between sex hormones and the gut microbes that live in your digestive tract. Gut microbes can influence hormone metabolism through enzymes such as beta-glucuronidase and hydroxysteroid dehydrogenase, while hormone changes can also shift the microbiome itself. This loop sits inside the brain-gut-microbiota axis, and it helps explain why gut microbiota and sex hormones may shape diarrhea, constipation, pain, and cycle-linked symptom shifts.
This overview is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, so you should seek medical guidance if symptoms are persistent, severe, or worsening.
How Do Estrogen, Progesterone, And Testosterone Affect IBS?
Hormones can change how fast your gut moves and how strongly it reacts in irritable bowel syndrome (IBS). The link between estrogen and irritable bowel syndrome often shows up as slower transit and more pain. Higher-hormone states can also line up with constipation-predominant IBS, bloating, and incomplete emptying. A classic review noted that sex hormones can shape motility and gut sensitivity in IBS (DOI).
A simple comparison helps:
Hormone | Main gut effect | Common IBS pattern |
|---|---|---|
Estrogen | Can shift pain signaling, immune activity, and serotonin handling | Cramps, urgency, nausea, or flares that do not always match stool form |
Progesterone | Strongly relaxes smooth muscle and slows transit | Constipation, bloating, and incomplete emptying |
Testosterone | May support steadier motility and lower pain sensitivity | Fewer flares for some people, though evidence is still limited |
Estrogen matters because it can change how your brain and gut read normal stretching. That is the heart of gut pain sensitivity in IBS, where ordinary bowel movement feels sharper or more painful than it should. In plain terms, visceral hypersensitivity and hormones can work together, so cramping, urgency, or pain may feel louder during hormonal shifts even when stool form barely changes. That kind of visceral pain modulation can also help explain symptom spikes around ovulation, the late luteal phase, or other times when hormones swing.
Estrogen also affects serotonin and immune signaling. The phrase 5-HT signaling IBS sex differences sounds technical, but the idea is simple. Serotonin helps the gut sense movement and coordinate bowel activity, while immune cells such as mast cells can make the gut more reactive when they are easier to trigger. In that setting, estrogen may amplify pain, nausea, or diarrhea-like urgency in people who already flare easily.
Progesterone is usually the stronger slowing hormone. In progesterone IBS patterns, smooth muscle relaxes more, transit takes longer, and the bowel has more time to absorb water from stool. That shift can push symptoms toward constipation-predominant IBS, especially when progesterone is relatively high compared with estrogen. The result is often slower, heavier-feeling digestion rather than a sudden stool change.
Barrier function adds another layer. The intestinal permeability estrogen story is still mixed in human studies, but estrogen may support tight-junction proteins such as occludin and junctional adhesion molecule A through estrogen receptor ER-α ER-β, especially estrogen receptor beta. When the gut lining is easier to irritate, small shifts in food, stress, or hormones can trigger more inflammation and a bigger symptom response.
Testosterone may act as a partial counterbalance. Lower androgen levels have been linked in some studies with more pain sensitivity, less steady motility, and more immune reactivity. That may help explain why some people notice more discomfort when androgen levels are lower, although the evidence is not as strong as it is for estrogen and progesterone.
Put together, the picture is less about one hormone causing IBS and more about a push-pull effect. Estrogen and progesterone often tilt toward slower transit, while hormone shifts that increase sensitivity, mast cell activity, or barrier leakiness can lean toward cramping, urgency, and looser stools. If your symptoms clearly follow your cycle, tracking stool form, pain, bloating, and timing can help you and your clinician decide whether hormone changes, hormone replacement therapy (HRT), or contraceptives deserve a closer look.
How Do Menstrual Cycle, Perimenopause, And Menopause Affect IBS?

Hormone shifts can make IBS louder at certain times of life, even when your diet stays the same. That pattern matters because it helps you separate a cycle flare from a new food trigger or a broader change in gut sensitivity. Tracking menstrual cycle IBS symptoms can turn a vague hunch into something easier to spot.
A review in the American Journal of Gastroenterology found that about 40% of women with IBS notice symptom changes across the menstrual cycle, while about one-third of women without IBS still report gastrointestinal symptoms during menstruation (DOI). Timing, in other words, can be useful evidence. It is not just a coincidence.
Life stage | What you may notice | Why it may happen |
|---|---|---|
Menstrual cycle | More belly pain, bloating, loose stools, constipation, or mixed bowel changes around your period | Estrogen and progesterone drop before and during menses, and that shift may reduce estrogen’s calming effect on the gut |
Perimenopause | Symptoms that feel less predictable from week to week | Estrogen and progesterone rise and fall unevenly, which can shift IBS toward constipation, diarrhea, or mixed patterns |
Menopause | Symptoms may ease, stay the same, or change shape | Monthly hormone swings end, but gut movement, pain signaling, and brain-gut communication can still affect symptoms |
The most common menstrual pattern is a flare around menses. Abdominal pain, bloating, and bowel changes often worsen when ovarian hormone levels are low. That can make a period-related flare look like a new food intolerance when it is really cycle-linked.
Perimenopause can feel even less predictable. Estrogen and progesterone no longer follow a steady monthly rhythm, so one week may bring constipation, the next diarrhea, and another a mixed pattern. If your periods are also changing in length, flow, or timing, the whole picture can get harder to read.
Menopause brings a different picture. IBS prevalence tends to decline after menopause, but improvement is not guaranteed. Some women feel better once monthly hormone swings stop, while more than one-third in one study still reported IBS-type symptoms. The gut can remain sensitive to stress, sleep loss, diet shifts, and other triggers.
Several forces may help explain why symptoms improve for some people and persist for others:
- Fewer hormone swings: Monthly estrogen and progesterone changes stop, which may reduce cycle-linked flares.
- Changed gut motility: Bowel movement speed can shift, and that can affect constipation, diarrhea, or both.
- Pain sensitivity changes: The gut may stay more sensitive even when periods are gone.
- Brain-gut signaling: Stress and nervous system responses still shape IBS symptoms after menopause.
A simple symptom log can make these patterns much clearer. Track pain, bloating, stool changes, and where you are in your cycle. That record can help you talk with a clinician about HRT or contraceptives, and it can also show whether premenstrual flares, new perimenopausal symptoms, or persistent postmenopausal symptoms need a closer look. Digestive symptoms can have many causes, so persistent, severe, or worsening symptoms deserve personalized medical advice, and results vary by person.
How Do Hormones Change Your Stool Patterns?
Hormones can make your stool pattern look less random than it feels. Estrogen and progesterone often slow gut movement, so stool stays in the colon longer and more water gets absorbed. That is one reason gut motility in IBS can shift across your cycle.
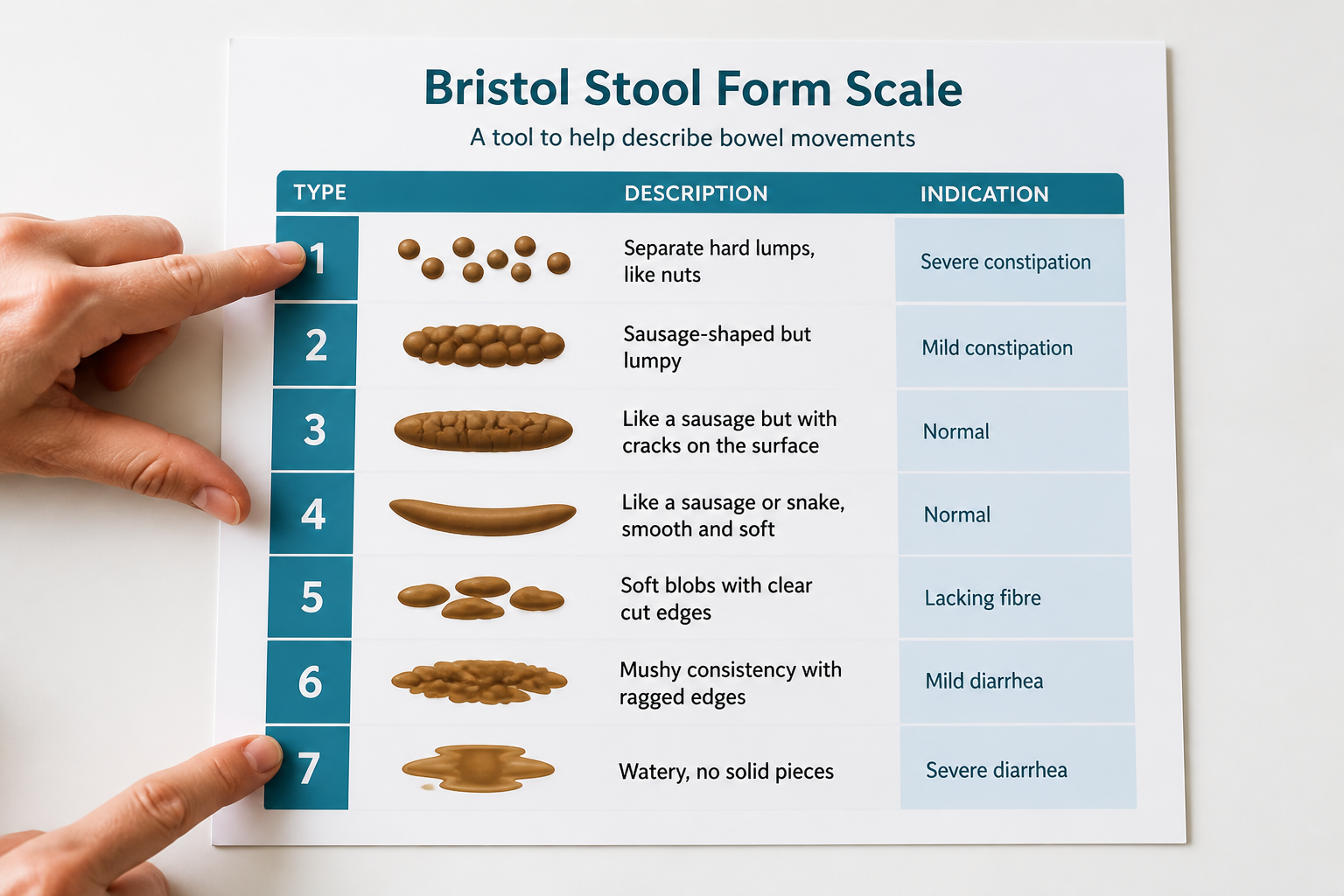
The Bristol Stool Scale helps you turn those changes into something you can track and describe clearly:
Bristol type | Usual meaning | What it often feels like |
|---|---|---|
Types 1 to 2 | Constipation pattern | Hard, lumpy stool, straining, incomplete emptying |
Types 3 to 4 | Typical formed stool | Smooth or soft formed stool |
Types 6 to 7 | Loose stool or diarrhea pattern | Mushy stool, urgency, frequent bathroom trips |
Type 7 means watery stool with no solid pieces. Physiology-wise, that usually points to very fast intestinal transit and less water reabsorption. Hormone-related flares, stress-related HPA-axis shifts, and other diarrhea triggers can all push stool in that direction. Older research on sex hormones and bowel function also helps explain why progesterone IBS patterns often lean toward slower movement (DOI00400-1)).
When hormone levels fall or change quickly, the picture can flip. Transit may speed up, stools can get looser, and urgency may show up with little warning. That is also why some people do not stay in one IBS category and instead move between constipation and diarrhea from week to week.
A simple pattern summary looks like this:
- Higher estrogen and progesterone states: slower transit, drier stools, more constipation-like symptoms
- Abrupt hormone changes: looser stools, urgency, or a mixed IBS pattern
- Stress surges and HPA-axis shifts: more cramping, diarrhea, or stool swings
That variation is real, and it helps explain why 5-HT signaling IBS sex differences matter. Serotonin helps regulate motility, and sex hormones can change how that signaling works. The same idea shows up in the enteric nervous system and sex steroids, where hormone signaling can affect stool form, pain, and bowel speed in different ways from person to person.
If your stool pattern changes with your cycle, track the day, stool type, and symptoms to spot a repeatable rhythm. This content is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes, so you should consult a qualified healthcare professional for persistent, severe, or worsening symptoms. Results vary by person, and any dietary or supplement advice should be individualized.
What Helps Calm Hormone-Related IBS Flares?

Hormone-related IBS flares often calm faster when you match the fix to the phase of your cycle. Estrogen and progesterone shifts can change gut movement, pain signaling, and stress reactivity. In some people, HPA axis dysregulation in IBS and CRF HPA axis IBS signaling make the gut extra jumpy before a period. The brain-gut-microbiota axis helps explain why symptoms can cluster even when your diet has not changed much.
A simple flare plan can look like this:
Flare pattern | What may help | Why it fits |
|---|---|---|
Symptoms that reliably show up before your period | Simpler meals, steady hydration, consistent sleep, and lighter activity for a few days | Lowers strain when your gut is more reactive |
Constipation-prone flares | A clinician may suggest timing fiber differently and keeping fluids steady | Can support stool movement without overwhelming your system |
Diarrhea-prone flares | Short-term antispasmodics may help when cramping is the main issue | Can ease spasm and make urgency feel less intense |
Severe IBS-D that keeps returning | A clinician may consider alosetron for women who meet strict criteria and need close supervision | Reserved for specific cases with careful monitoring |
A short low-FODMAP window is usually more useful than staying restrictive all month, because clinical guidance uses the diet as a temporary elimination phase before foods are reintroduced (source, source). That means using it only during your worst hormone-sensitive days, then widening food choices again as the flare settles. In one randomized crossover feeding trial in women with endometriosis and gastrointestinal symptoms, about 60% responded, with better abdominal pain and quality of life (DOI).
If the same meals seem to hit hardest in the same phase, identifying IBS food triggers can be part of the picture too. Short-term antispasmodics can help when cramping is the main complaint. For severe IBS-D, a clinician may consider alosetron or another serotonergic agent when you meet strict criteria and need close supervision.
Stress care belongs in the flare plan, not after it. Hormone shifts can interact with the HPA axis and the body’s stress circuits, and symptoms may worsen when cortisol-related signaling stays high. The brain-gut-microbiota axis also helps explain why sleep loss or a tense week can make a cycle flare feel louder than it should.
These small resets are often the easiest place to start:
- Slow your breathing for a few minutes when pain or urgency rises.
- Choose paced walks instead of hard workouts on flare days.
- Cut back on caffeine if it makes urgency, jitters, or cramps worse.
- Keep a predictable bedtime routine so sleep stays steady.
A symptom log by cycle phase can make the next flare easier to predict. Write down the day symptoms start, stool pattern, urgency versus constipation, and any repeated food or stress triggers. That record helps separate hormone-linked flares from other causes and shows whether diet changes or medicine should be timed earlier. It also gives your clinician a clearer map if symptoms keep cycling.
Seek prompt medical care if any of these show up:
- Severe or worsening abdominal pain
- Dehydration or trouble keeping fluids down
- Blood in the stool
- Fever
- Fainting or near-fainting
- Unexplained weight loss
- New nighttime symptoms that wake you up
- A major change in your usual IBS pattern, especially if it keeps lining up with your cycle
This content is for educational purposes only and is not a substitute for personalized medical advice. Digestive symptoms can have many causes. You should consult a qualified healthcare professional for persistent, severe, or worsening symptoms. Results vary by person, and any dietary, supplement, or medication advice should be individualized.
When Should You Talk To A Doctor About HRT?
If your IBS symptoms begin or noticeably worsen after starting hormone replacement therapy, bring it up at your next follow-up instead of brushing it off as a random flare. That matters most when the change is new, persistent, or getting in the way of work, sleep, or meals. The timing can be a real clue in hormone replacement therapy and IBS, even when it is not the whole explanation.
The strongest cohort evidence points to a possible link, not a proven cause. In one cohort study of women ages 50 to 69, confirmed IBS occurred at 3.8 cases per 1,000 person-years in the HRT group and 1.7 cases per 1,000 person-years in the comparison group, which indicates a higher incidence in HRT users (source). The same research also fits a broader pattern in which IBS in women tends to decline with age and move closer to male rates after age 70 (source).
That does not mean HRT causes IBS for everyone. It does suggest that hormones can shape gut symptoms in some people, which is why HRT and IBS often come up together in clinic visits. A few plausible pathways may help explain the pattern:
- Gut motility: hormone shifts can speed up or slow down how fast stool moves.
- Visceral sensitivity: the bowel can become more pain-sensitive or more reactive.
- Brain-gut signaling: hormone changes and stress signals can interact and shift bloating, urgency, or cramping.
Older suppression studies, including work using the GNRH agonist leuprolide, also support the idea that ovarian hormone changes can alter symptom patterns in sensitive people (source).
When you talk with your clinician, keep the conversation concrete. It helps to ask whether your symptom pattern lines up with the start of HRT, whether a different dose or formulation might matter, and how to balance menopause relief against possible digestive side effects. It is usually better not to stop treatment on your own.
These changes deserve prompt medical review:
- Worsening pain
- Blood in the stool
- Unexplained weight loss
- Vomiting
- Anemia
- Fever
- A major change in bowel habits
Digestive symptoms can have many causes, so persistent, severe, or worsening symptoms should be assessed by a qualified healthcare professional. This content is for educational purposes only and is not a substitute for personalized medical advice. Results vary by person, and any dietary or supplement advice should be individualized.
Hormones In IBS FAQs
Questions about hormones in IBS often focus on how the menstrual cycle, perimenopause, and menopause can change symptoms from one person to the next. The family history and IBS link adds another layer to that picture. The IBS after infection link and epigenetic modulation microbiome shifts help explain why patterns differ.
1. What Hormone Imbalance Can Trigger IBS?
The most plausible IBS hormonal triggers are rising or swinging estrogen, low or unstable progesterone, and stress-related cortisol changes. Estrogen shifts can be more noticeable in IBS-D because they may increase visceral hypersensitivity and hormones-related gut signaling, while lower progesterone may matter more in IBS-C because it can affect visceral pain modulation, slow motility, and add bloating through TRPV1 TRPM8 IBS pathways. Testosterone findings are mixed, but lower levels may raise symptom sensitivity in some people, and cortisol is not a sex hormone, yet chronic stress can make it more reactive and worsen pain, urgency, and bowel instability across subtypes (DOI).
2. Why Do IBS Symptoms Worsen Before Periods?
IBS often flares in the late luteal phase, just before your period. Those hormone shifts can slow or make gut transit less predictable, so you may notice constipation, looser stools, or more urgency depending on your usual IBS pattern. Changes in mast cells may add to inflammation and sensitivity in irritable bowel syndrome. These menstrual cycle IBS symptoms are common, but persistent or severe changes still deserve medical review.
3. Can Hormone Therapy Change IBS Symptoms?
Hormone replacement therapy and IBS can be linked, but the pattern varies by person and treatment plan. Some studies suggest HRT and IBS risk may rise rather than symptoms reliably improve, and that signal has appeared with both oral and transdermal routes, plus different regimens and lengths of use. Your baseline IBS risk, hormone history, and the specific plan all shape whether symptoms improve, worsen, or stay steady, while the way hormones affect the gut is still being studied. Findings from GNRH agonist leuprolide also suggest hormone shifts can change gut sensitivity.
4. What Is Type 7 IBS Stool?
Type 7 on the Bristol Stool Form Scale usually points to very fast colonic transit rather than normal stool formation. In hormone-related IBS, your colon may move stool through too quickly to reabsorb much water, so it stays loose. Hormone shifts can also affect serotonin signaling in the gut, which may raise secretion and bowel activity. Occasional Type 7 stool can happen during flares, but frequent or worsening watery diarrhea should be discussed with a qualified healthcare professional, especially if you have pain, dehydration, or weight loss.
